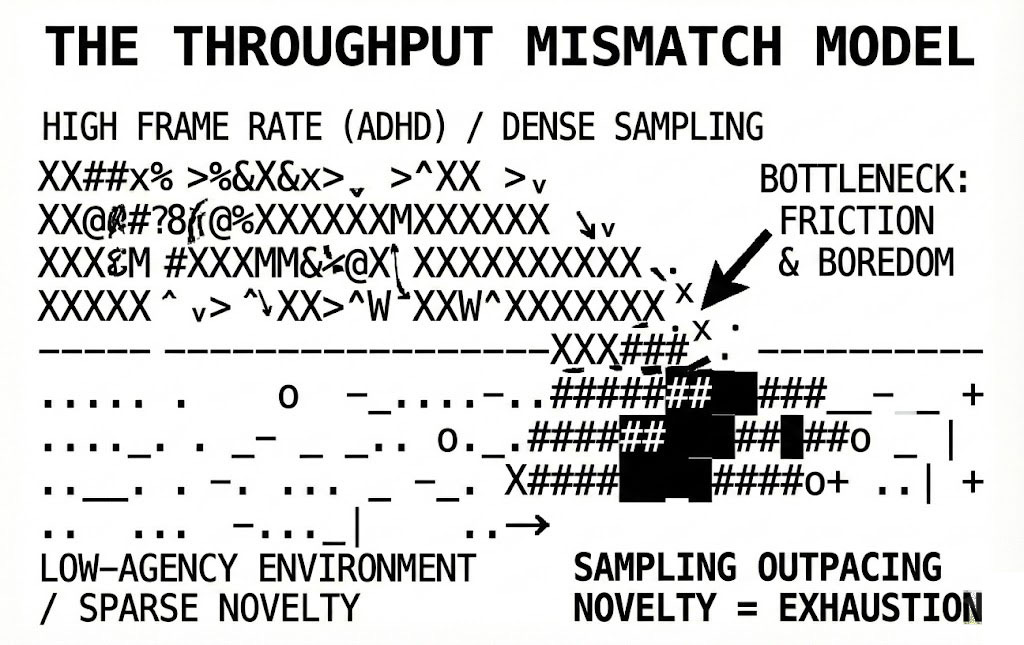
"experiencing reality at a high frame rate" is how I've often described my experience & potentially the experience of adhd broadly
both your perceptual sampling rate (experiencing shifts in sensory inputs and/or internal states) AND agency sampling rate (opportunities/affordances to act on something) tend to be higher, which is precisely the reason why you get bored, exhausted, jaded faster
- orpheas
One of the magical things about social media is that like a diffusive process, sometimes someone will accidentally strike the heart of a place that everyone else seemed to miss. When Orpheas laid his claim about attention yesterday in response to Scott Stevenson’s longer post on the same, I first thought to seek clinical information either repudiating or validating his argument. What I found was far more interesting, and eventually metastasized into the article you’re reading.
The phrase “experiencing reality at a high frame rate” seems to have emerged from years of trying to articulate something the clinical literature dances around but never quite names (something common in medical research, which over the past four years, I have read an unbelievable amount of). I’m not a doctor nor a healthcare professional, but I’m also no stranger to this. I’ve read every single PubMed accessible article on eosinophilic granulomatosis with polyangiitis (EGPA) since 2021, most of the research literature on GLP-1’s and IL-5, IL-13, and IL-8 modulating immunotherapies since 2022, and various published works on longitudinal studies related to COVID-19 since 2020. Every week, almost every day, agent systems I’ve developed for this task search for new literature hoping that someone will announce a P1 clinical trial for a new immuno-modulating biotherapy which inches me closer to ‘curing’ EGPA, FDA be damned. And so far, I’d say the results have been good — in combination, of course, with medical oversight, which I selectively hide only the most confusing details from.
As for differences in temporal perception, and unlike causative factors for ‘ultra-rare’ disorders like EGPA, the research is there. There are dozens of papers confirming that ADHD involves measurably different temporal processing. Much like a rare disease or new treatment, the phenomenology gets lost in operationalization. What does it actually feel like to have an accelerated internal clock?
Let’s start with the basics. Smith et al. (2002) found children with ADHD needed intervals approximately 50 milliseconds longer than controls to discriminate between durations: a perceptual deficit at the threshold of conscious experience. Toplak and colleagues extended this across modalities: auditory, visual, subsecond, suprasecond. More evidence here, here, here, here, and so on. Despite differences in perception across modalities, the effect persists. Zheng’s 2022 meta-analysis of 27 studies landed on a Hedges’ g of 0.66 for timing precision (a medium-to-large effect that doesn’t wash out across paradigms). Marx et al. (2022) synthesized 55 studies and confirmed what everyone suspected: ADHD involves an accelerated internal clock. The pacemaker ticks faster. Subjective seconds take longer to pass. Time just hits different.
This is where most reviews stop. “Time perception deficit.” Noted. Wrong buzzer noise. Big neon sign that reads, “DEFECTIVE”. Moving on. Nothing to see here.
But the frame rate metaphor captures something the clinical framing misses entirely. When your internal clock runs faster, you don’t just perceive time differently — you sample reality at a higher rate. It could be argued that this means someone with this diagnosis takes more perceptual snapshots per objective second. More shifts in sensory input registered. More micro-changes in internal state noticed. The literature describes this as “elevated discrimination thresholds” and “greater within-subject variability.” To the observer, it’s almost like the world moves in slow motion and you’re stuck watching every frame.
You can imagine how most places in America are not optimized for this type of perception. You can also imagine that most people within 2 standard deviations of the middle of the sample-rate bell curve will be incapable of relating to it. You can also assume that being a child (increasingly subject to low-agency environments), experiencing this, and trying to articulate it to adults (who may likely also be dumber than you, especially if they are choosing to exist in low-agency environments) can be extremely frustrating up to completely devastating to the actor.
This leads folks like Orpheas and I to the piece that doesn’t show up in the neuropsychology journals (yet): agency sampling rate. To “steelman” Orpheas’ argument: if you’re registering more moments per unit time, you’re also registering more choice-points per unit time. This means you have more affordances, more opportunities to act. More micro-decisions about whether to engage or disengage, pursue or defer, speak or stay silent. If you’re thinking of life in terms of decision trees, this means you can see smaller branches. The map, as compares to a raster image, has more DPI.
Sonuga-Barke’s delay aversion work gets close to this. The 1992 study established that hyperactive children don’t just prefer immediate rewards, they actively escape from delay itself. The delay is aversive independent of the reward structure. Jackson and MacKillop’s 2016 meta-analysis (3,913 participants, d = 0.43) confirmed steeper delay discounting curves across the board. But “delay aversion” frames this as pathology: you can’t wait, you’re impulsive, you lack self-control.
By de-contextualizing the connection between attention sampling and agency, I argue that medical professionals may be predisposed to argue that anything outside the norm is at least pathological and at most dysfunctional. My personal theory as to why this happens is because more primitive civilizations (on a mid-level, those in America which exist outside major economic trade hubs, educational/medical/intellectual density points, and like it or not — large urban centers) are functionally unequipped to provide enough agency-options within their environment to satisfy the needs of those with higher sampling rates. The most they can produce are complex simulacra of meaning. Public health is designed to follow optimal patient outcomes, and some places are very bad at producing good outcomes for out-of-distribution actors.
One physical example of this is Orlando, FL: the city I was born in. At one point in the 60s and 70s, it was well on the way to becoming one of the first places in the world to produce a Socialist network state. The plans were vast and shocking: a new prototype community of tomorrow which would meet the economic, educational, medical, and leisure needs of an increasingly wealthy suburban population by bootstrapping a dense, climate-controlled city with private capital. The Reedy Creek Improvement District captured autonomy from state control and made the very idea possible. Until very recently, Disney (or its parent city, Lake Buena Vista) could operate its own spaceport and nuclear reactor. Today, the RCID (inked into reality by Claude Kirk) has been disbanded and replaced with the Central Florida Tourism Oversight District, which is currently led by three individuals: one in real estate, a chair of a low-performing local college, and the owner of the private company which contracts with Disney to operate its buses. This group is advised by a group of pastors with no urban planning or technological experience whatsoever.
As Walt Disney’s original vision for EPCOT fell victim to Roy O. Disney’s desire to commercialize the idea, the result today is a city which is quite different than what was originally envisioned: one in economic and intellectual decline. It has failed at any point in its history to produce a Fields medal recipient, does not contain nor is adjacent to any medical or technological capacity besides that which is required at the bare-minimum level of service (aside from companies like Boeing and Lockheed Martin which arguably trail behind companies like SpaceX and Anduril), looking more like a landlocked city than the coastal economies which flank it to the East and the Southwest, (Tampa and Miami). Orlando’s #2 employer: Advent Health, follows the pattern of nearly every state in the US (healthcare is the #1 employer) while operating in a worse market and suffering from structural inefficiencies (Florida as a whole ranks around 38th in healthcare). The number one employer is the primary driver of tourism in Orlando: Walt Disney World resort. The number three employer is Universal Studios. What exists downstream of the parks is a cottage industry of slowly decaying tourist traps and a few independent resorts. Hospitality second to the tourist economy. It now costs less for an American to travel internationally to Japan, including room and airfare, to visit Disney in Toyko than it does for them to visit EPCOT in Orlando. Generally speaking, this does absolutely nothing to prevent more ‘brain drain’ from happening as many young people continue to leave towns like these for larger cities and broader economic opportunity (a global and historical phenomenon). So, why design and administrate a place like this? My theory is actually quite simple: Ph.D. recipients or high-agency independents like startup founders don’t make good resort workers & do not natively stimulate tourism. Education is the ticket out. In this way, higher-agency systems like “broadening your worldview by moving somewhere new to live / study / work” collapse the ability for these places to function as they currently do. This is why many places in America have social and political mechanisms in place to keep things the way they are. It likely comes from the places themselves, especially those which are failing to adapt to demographic, environmental, territorial, and information-landscape changes.
Large swaths of America (and global medical literature) still frame differences in attention, especially in low-agency environments, as pathological and something to be cured on the individual level than accounted for in the wider structure of the info-environment. If you exist out of the middle 2-standard-deviation band of the bell curve, it’s a you problem, and not a structural-environmental problem, where your surroundings are not properly structured to provide enough agency. This kicks people with higher attention sampling rates out of being able to meaningfully engage with and ultimately change their surroundings, and compounds the problem of places not being built for high attention sampling rates on a systemic level.
So, what if the frame rate model inverts this? Let’s say instead — you’re not failing to tolerate delay — you’re just experiencing more of it. If your internal clock samples at 1.3x the rate of neurotypical clocks, a five-minute wait contains 6.5 minutes of subjective duration. But more importantly, it contains ~30% more moments where you could act and don’t. Each of those moments accumulates as friction. The wait isn’t just longer; it’s denser with unchosen choices. The pressure is higher because you are noticing more often.
i-a. BOREDOM IS SAMPLING OUTPACING NOVELTY.
i-b. EXHAUSTION IS ACTING ON TOO MANY AFFORDANCES.
i-c. JADEDNESS IS PATTERN-COMPLETION RENDERING SAMPLING REDUNDANT.
We have now re-engineered the ADHD experience as a throughput problem rather than a capacity problem. Framing it as a problem, that you ‘can’t sustain attention’, is now the incorrect vantage point. Instead, we claim that your attention samples the environment at a rate that exceeds the environment’s novelty generation. Now consider the difference in outcomes for urban environments: ones with green spaces and complex navigation stave off Alzheimer’s and dementia, compared to suburban and rural environments, affecting downstream QoL and ultimately life expectancy. These issues matter, they affect people’s lives and the people they ultimately become.
Suddenly, boring meetings aren’t boring because you lack focus; they’re boring because you’ve extracted all available information by minute three and your clock keeps ticking for the remaining fifty-seven.
Church isn’t boring because you’re a heretic, it’s because the information is presented from a fixed corpus. The interpretation may change, but the system is a closed-loop system.
The research on fMRI during timing tasks is suggestive here. Hart et al. (2012) found reduced activation in left inferior prefrontal cortex and cerebellum during timing, but increased activation in posterior cingulate and precuneus (the default mode network). The ADHD brain isn’t shutting down during under-stimulating tasks. It’s redirecting processing toward internal simulation. If the external environment isn’t generating enough novelty to match sampling rate, the system starts generating its own. Your surrounding world is insufficient, so they must dream their own. Bootstrapping the training of a world-model with synthetic data, which is exactly how open-source LLM companies develop their own models. It takes the open-source Chinese labs around 7 months to catch up to the closed-source frontier labs.
Walg et al. (2017) found something interesting: processing speed correlated with estimation accuracy only in the ADHD group. Slower cognitive processing partially compensates for faster clock speed. This suggests a possible equilibrium state—high-processing-speed ADHD might be functionally different from low-processing-speed ADHD. For example: two people with ADHD has the same accelerated clock, but a different ability to act on the affordances it generates.
ii. HIGH-AGENCY ENVIRONMENTS ARE LESS EXHAUSTING THAN LOW-AGENCY ONES.
The triple pathway model (Sonuga-Barke et al., 2010) established that timing, inhibition, and delay-related impairments are statistically independent in ADHD —separate pathways to the same diagnosis. But what if timing is upstream of the other two? An accelerated clock generates more perceived choice-points. More choice-points generate more inhibition demands. More inhibition demands generate more delay (between impulse and action). This clearly means the pathways aren’t parallel. It defines them as cascading.
This would map that high-agency environments — contexts where acting on perceived affordances is actually appropriate — should be paradoxically less exhausting for ADHD individuals than low-agency environments with equivalent stimulation levels. The crisis/high-stakes pattern fits this: it’s not that ADHD brains need stress, it’s that high-stakes contexts justify the agency sampling rate. When every perceived choice-point actually matters, the friction disappears. The frame rate matches the action rate.
Noreika, Falter, and Rubia’s 2013 review (32 pages, the definitive synthesis) noted that timing deficits survive when working memory, attention, and inhibition are controlled for. Timing is foundational. But they didn’t extend the logic to agency. They never proposed the idea that temporal perception directly modulates the density of possible action in any given span of experience.
iii. THE DEFICIT MODEL DESCRIBES MISMATCH AS PATHOLOGY.
The dopaminergic story makes this even cleaner. Jones and Jahanshahi (2011) reviewed how phasic dopamine signals interval onset/offset while tonic dopamine alters internal clock speed. Dopamine agonists cause time underestimation (faster clock); antagonists cause overestimation (slower clock). Methylphenidate normalizes both behavioral timing and neural activation patterns (Rubia et al., 2009). The pharmacology confirms the mechanism. Anticipate alongside the Cambrian-esque explosion of grey-market peptides, and the popularity of pharmaceuticals like modafinil amongst military and intelligence elites, that there will be an increasing number of chemical options for increasing your attention sampling rate in 2026 and into 2027 and beyond. Previous to the hyper-individualist now, we used to do this through corporate structure & systems engineering. Now, these have decayed into oxidized machines designed to keep the least observant comfortable at the expense of people outside of their perceptual-peripheral vision.
Normalization clearly isn’t the same as optimization. If you’ve built your entire cognitive style around high-frame-rate processing, your expertise, like pattern recognition, creative approach all depend on sampling reality more densely than baseline, then slowing the clock might solve the friction problem while creating a different one. Now you’re not experiencing delay aversion anymore, but you’re also not seeing what you used to see. Your perception of time is blurry. This is fundamental to the way low-agency environments & places iron out perceptual differences. You have to be able to not tell how much time has elapsed. Endless nostalgia is a symptom.
iv. WHAT YOU CALL DEFICIT I CALL MISMATCH.
v. WHAT YOU CALL MISMATCH I CALL NICHE.
The question isn’t whether ADHD involves temporal processing differences. The research is unambiguous (it does). The question is whether those differences are uniformly costly or whether they’re costly only in environments that don’t match the sampling rate.
Waiting rooms. Lectures. Orlando. Any context where the appropriate action is “sit still and receive information at a rate determined by someone else.” These are low-affordance environments experienced at high frame rate — and it feels like surveillance of your own life, as I put it earlier.
The boredom isn’t lack of interest.
It’s attention repeatedly activating in a context where activation can’t be exercised, released from the body, exhaled as carbon dioxide against the oxygenated fresh breath of novel input.
vi. THE CURE FOR BOREDOM IS NOT STIMULATION.
vii. THE CURE FOR BOREDOM IS PERMISSION.