Specialization in medicine drove most of the dramatic health improvements of the last 100 years
But now we've overspecialized our medical system; care is fragmented and expensive. More specialization won't help.
Recent technical advancements that bring expert knowledge to generalists and patients at scale have the potential to fix this problem
Before urbanization, all doctors were generalists—delivering a baby in the morning and treating pneumonia in the afternoon. The idea that you could choose to treat only one specific type of medical issue was impractical at the time.
With cities came the ability to specialize. Obstetricians no longer performed amputations. Doctors could focus on one aspect of human health, seeing far more cases in their specialty than any generalist could. This concentrated expertise allows specialists to follow patient outcomes more closely, notice subtle patterns, understand how patient differences affect outcomes, and innovate based on larger sample sizes.
Specialization in medicine drove fantastic outcomes. Infant mortality plummeted over 90% from 100 per 1,000 births in 1900 to under 7 by 2000, with the steepest declines following the establishment of pediatrics as a specialty. As anesthesia became its own specialty, instead of a responsibility of general surgeons or doctors, mortality rates under anesthesia dropped 100-fold.
Specialists contribute in two ways: they innovate because they can dedicate their full attention to solving specific problems, and they excel through repetition—performing the same procedures until they achieve mastery.
Complex procedures show 2-3 times higher mortality when performed by low-volume surgeons versus high-volume specialists. Specialization is a proxy for volume; volume drives pattern recognition and better outcomes. Surgeon mortality rates are inversely related to case volume across all procedures—the adjusted odds ratio for operative death ranges from 1.24 for lung resection to 3.61 for pancreatic resection when comparing low-volume to high-volume surgeons.
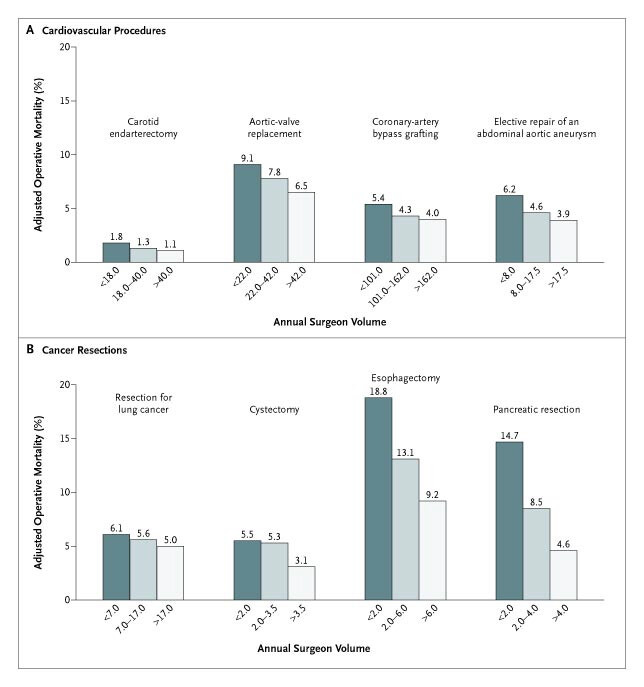
5-year survival rates for cancer patients at specialty cancer centers are 53% versus 44% at community hospitals.
The doctors at Sloan Kettering are likely more experienced, but critically they're also more specialized. The oncologist on your tumor board has seen perhaps 100x more patients with your specific cancer type than a rural general oncologist. That disparity means 100x more opportunities to refine their clinical decision-making through real-world feedback.
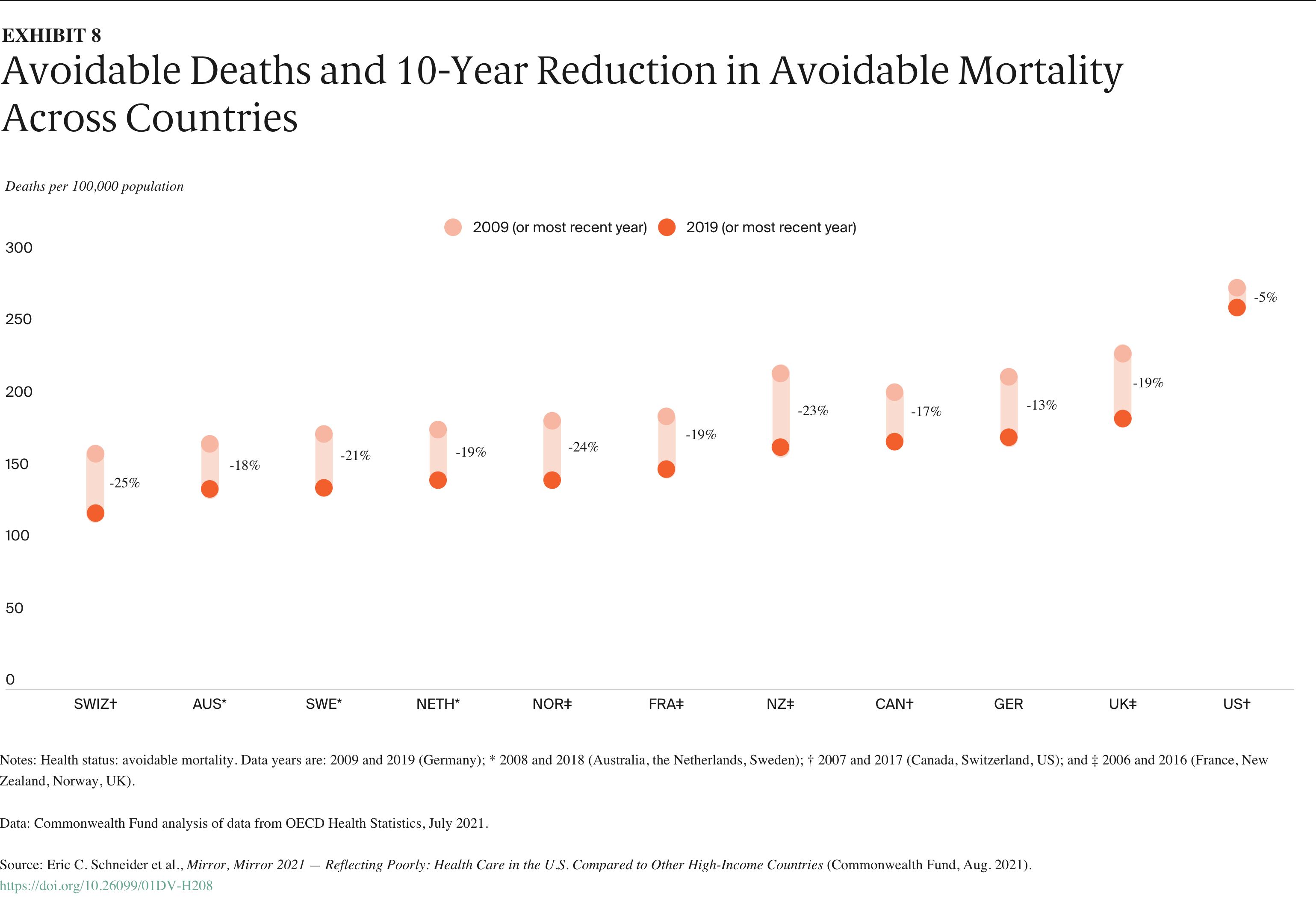
But evidence suggests that we may have reached diminishing returns on human specialization. The U.S. has a 2:1 specialist-to-generalist ratio—one of the highest in the world—yet demonstrates poorer health outcomes than countries with stronger primary care systems.
We’re hitting a wall in improving our quality of care.
A large contributing factor is care fragmentation. Patients shuttling between multiple uncoordinated clinicians, often repeating tests and receiving conflicting treatment plans. A Danish study of 4.7 million patients found that highly fragmented care—seeing multiple specialists without coordination—increased mortality risk by 2.59 times, even after adjusting for disease severity. In the U.S., 30% of Medicare beneficiaries see five or more physicians annually, creating communication breakdowns and treatment conflicts.
Despite evidence that fragmentation worsens outcomes, hospitals keep adding specialists. Largely because of financial incentives.
The way we’ve set up our healthcare system encourages care to take place in hospitals, by specialists. And hospitals have gotten way more consolidated in the last 30 years, mostly through regulatory capture.
Notably, the Affordable Care Act sharply limited Medicare participation and expansion of physician-owned hospitals. These physician-owned facilities had consistently outperformed traditional hospitals on quality, efficiency, and cost.
Between 2007 and 2013, the number of physicians employed by hospitals nearly doubled from 96,000 to 182,000. When hospitals acquire physician practices, they can immediately increase billing through site based billing. Medicare pays significantly more for services performed in a hospital setting. And specialists bring in almost 3 times more revenue per clinician than PCPs. Hospital margins have increased significantly through consolidation and specialization, which has been a major driver for total healthcare spending.
The same specialization that improved medicine now drives revenue through fragmentation. Hospitals will find it challenging to reduce fragmented care—the financial incentives all point the other way.
Hyper-specialization creates cascading access problems. Patients can't find the appropriate specialist for their condition. A patient with joint pain must navigate between rheumatologists, orthopedic surgeons, sports medicine physicians, and pain management specialists—multiple consultations before finding care.
Wait times compound with specialization. Pediatric rheumatologists average 3-6 month wait times; some subspecialties lack practitioners in every state.
The training pipeline cannot scale to this. Subspecialty fellowships now extend training to 7-10 years post-medical school. The narrower the specialty, the fewer doctors we produce.
To maintain the quality that specialization brought medicine, specialization must shift from practitioners to systems.
AI tools already augment generalist capabilities. Google's diabetic retinopathy algorithm enables primary care clinics to screen for vision loss with specialist-level accuracy. Point-of-care ultrasound with AI allows emergency physicians to obtain cardiac scans previously requiring sonographers. ECG interpretation algorithms identify atrial fibrillation with cardiologist-level accuracy, enabling immediate treatment decisions in primary care.
Clinical decision support systems transform pattern recognition. Mental health platforms analyze speech patterns and behavioral data to flag depression severity, providing psychiatrist-level assessments to counselors and general practitioners. These tools don't replace clinical judgment—they augment it with pattern recognition derived from populations no single specialist could observe.
Many of these tools are FDA-cleared for specific uses—typically detection or triage—not full diagnosis. Clinicians remain responsible for medical judgment and treatment decisions.
Rather than choosing between generalists and specialists, the approach involves providing generalists with access to specialist-level pattern recognition through systems that have learned from more cases than any human specialist could see in a career. Doctors can focus on building relationships that drive adherence, navigating complex decisions with patients, and coordinating care.
Specialization saved medicine by concentrating expertise. Now we can embed that expertise in systems accessible to both doctors and patients. Your primary care physician can access specialist-level pattern recognition for complex conditions. You can get dermatologist-quality skin assessments from your phone. We need specialist knowledge everywhere, available to everyone who needs it.