Whenever I give a public talk - after I’ve finished explaining how neuroscientists can now selectively manipulate or erase a mouse’s memories, or how patients sometimes have their heart and brain activity entirely stopped during surgery by cooling them below 20°C - and I’ve finished making the case for preserving the brains of dying people so as to give them a chance of future revival, I’m inevitably asked the following question during Q&A:
“OK, but what do your colleagues think?”
It’s a good question.
When I say ‘brain preservation may be able to stop people from dying’, I’m making a weird, bold claim. Weird, bold claims are mostly wrong. Still, if the claim is being espoused by a community of relevant experts - rather than just a few enthusiastic advocates - it’s much more likely to be worth taking seriously.
Of course, in an ideal world, I wouldn’t need to cite expert opinion at all; I’d just be able to show you unambiguous evidence of the procedure working, from preservation through to revival. I dream of the day when the first revived laboratory mouse - revived from cryogenic temperatures, or uploaded into a robotic murine body - runs through a maze just as it did before it was preserved. (Perhaps perversely, I would even appreciate some definitive proof that preservation cannot work - at least then we’d know this avenue was closed, and could turn our efforts elsewhere.)
But preservation is a two-part technology. The preservation half happens now; the revival half happens (maybe) in the future. We can’t run the full experiment just yet. For now, we’re stuck doing what we do for any consequential question where we can’t just wait and see (as with climate change projections or assessing the trajectory of AI development): we gather the best available evidence, and we ask the people most qualified to interpret it.
So, to return to my perennial audience question then, what do my scientific and medical colleagues think of the prospects of preservation?
Last year, Andrew McKenzie, Emil Kendziorra, and I surveyed 312 neuroscientists about the neurophysiological foundations of memory and whether preservation could enable indefinite memory retention. We found the typical respondent believed there’s a 40% probability that a well-preserved brain retains its long-term memories and could eventually be uploaded1 (publication, blog post, news article).
This year, we turned to the medical community. Using Sermo, an online survey platform for healthcare workers in the US, we asked 334 doctors how likely preservation is to work, whether they’d endorse medical interventions that could improve preservation outcomes, and what they thought about the ethics of the whole enterprise.
If you’re a nerd, here’s the preprint, the survey, and the raw data. Otherwise, read on for a summary.
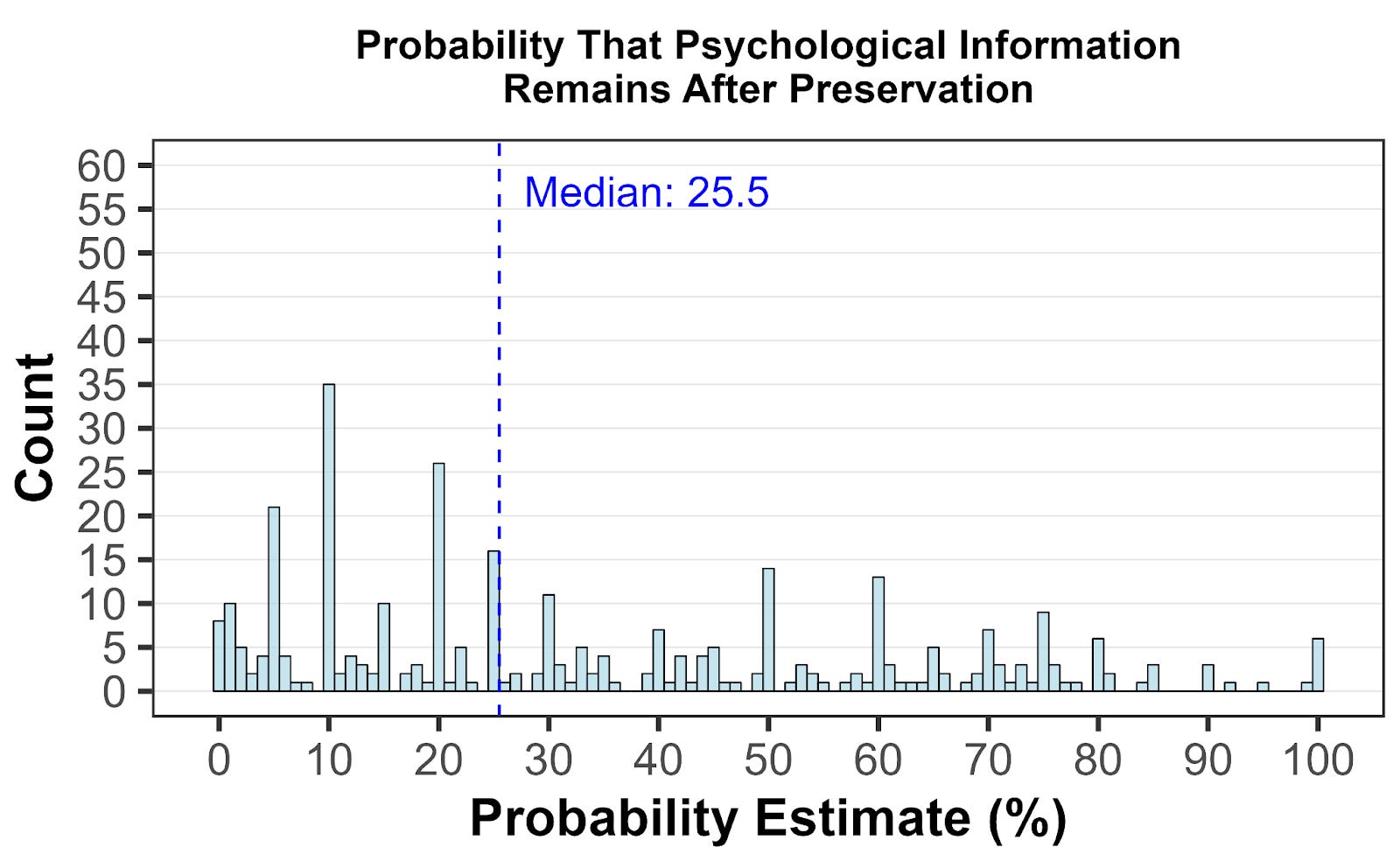
Our central question was how likely doctors thought preservation was to actually work. To assess this, we presented them with an idealised scenario: an elderly patient who wanted preservation, who suffered a cardiac arrest, and who was preserved within minutes. Follow-up imaging and biopsies confirmed intact brain structure down to the synaptic level. Given all that, how probable did they think it was that this patient could eventually be revived?
The median response was 25%.
We also asked the question more qualitatively: “How plausible do you find the idea that preservation could potentially allow for some form of revival in the future?” Here, 27.9% of respondents found it somewhat or very plausible, while 47% found it somewhat or very implausible. The remaining quarter were neutral - which, given the uncertainty involved, seems fair enough.
When we broke the probability estimates down by specialty, nothing dramatic emerged. Neurosurgeons were slightly more optimistic, palliative care doctors slightly more pessimistic, but medians hovered between 20-30% across the board. (We weren’t really powered to detect subtle specialty differences anyway, so I wouldn’t read too much into the variation.)
Believing preservation might work is one thing. Being willing to help make it work is another.
A patient’s chances of high-quality preservation depend heavily on whether their doctors are willing to support the process. A lot can go wrong, but one particularly pernicious problem is clotting: blood begins to coagulate quickly after cardiac arrest, blocking the vessels needed to carry cryoprotectants or fixatives into the brain. Administering anticoagulants like heparin before death can help reduce this problem.
We asked doctors whether it should be allowable to prescribe heparin to an imminently terminal patient who wants to be preserved. 70.7% said yes; only 11.7% opposed.
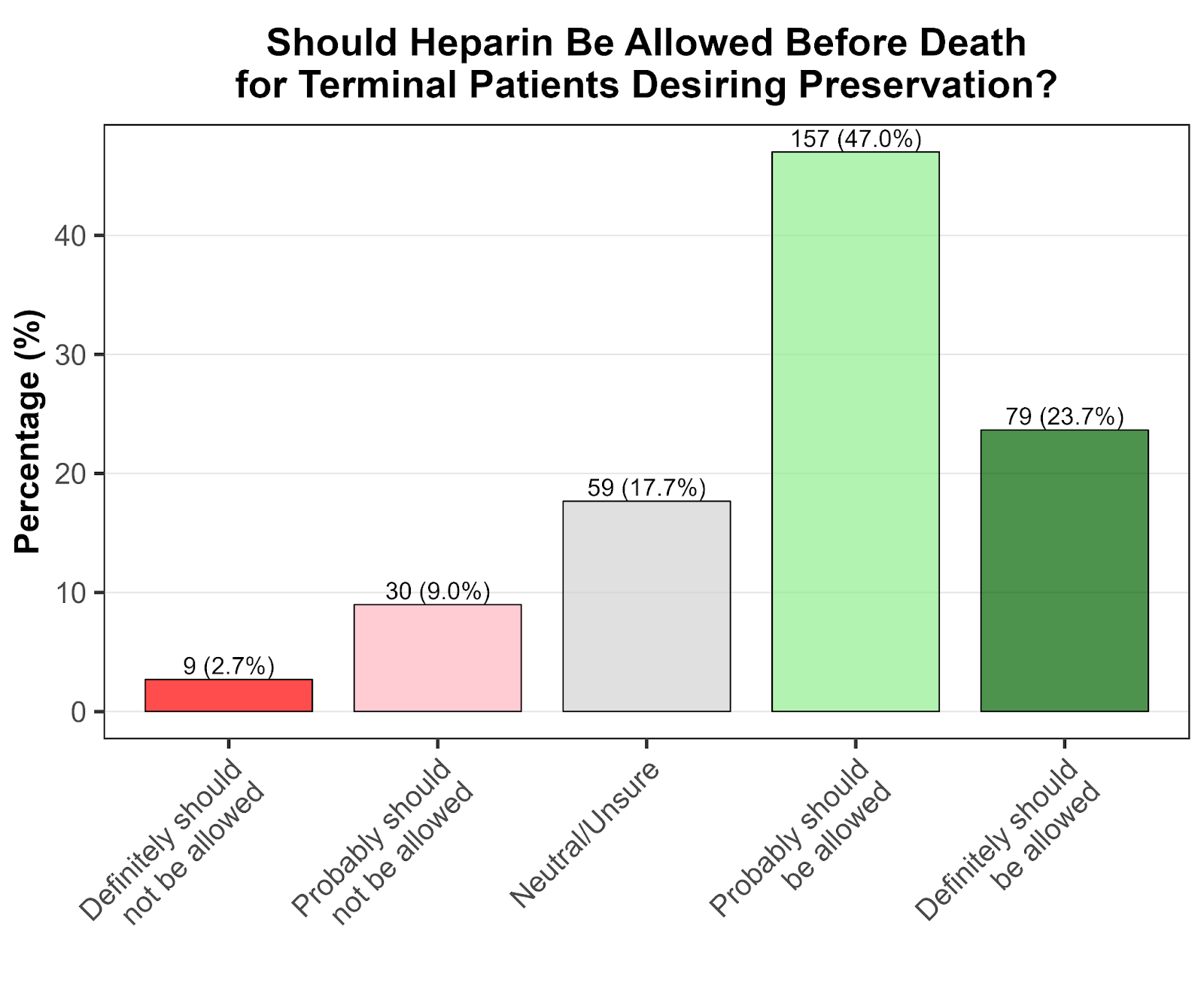
This was encouraging, though perhaps not surprising - anticoagulants are already routinely administered with minimal side effects, so this isn’t asking doctors to do anything too unusual.
The more controversial question involves timing. Currently, preservation procedures can only legally begin after cardiac arrest and declaration of death. But this delay - even if only minutes - significantly compromises preservation quality compared to animal studies, where procedures begin under deep anaesthesia while the heart is still beating.
This matters most for patients who want to be preserved but have also chosen medical assistance in dying (MAiD). Given they’ve already decided to end their lives, they’re going to legally die regardless. The question is whether preservation can begin in the brief window after they lose consciousness but before their heart stops.
We laid out this scenario explicitly: a terminally ill patient chooses MAiD, requests preservation, takes the medication, and loses consciousness. Should it be legal to begin preservation now, while the heart is still beating but death is inevitable and imminent? Or must we wait for cardiac arrest?
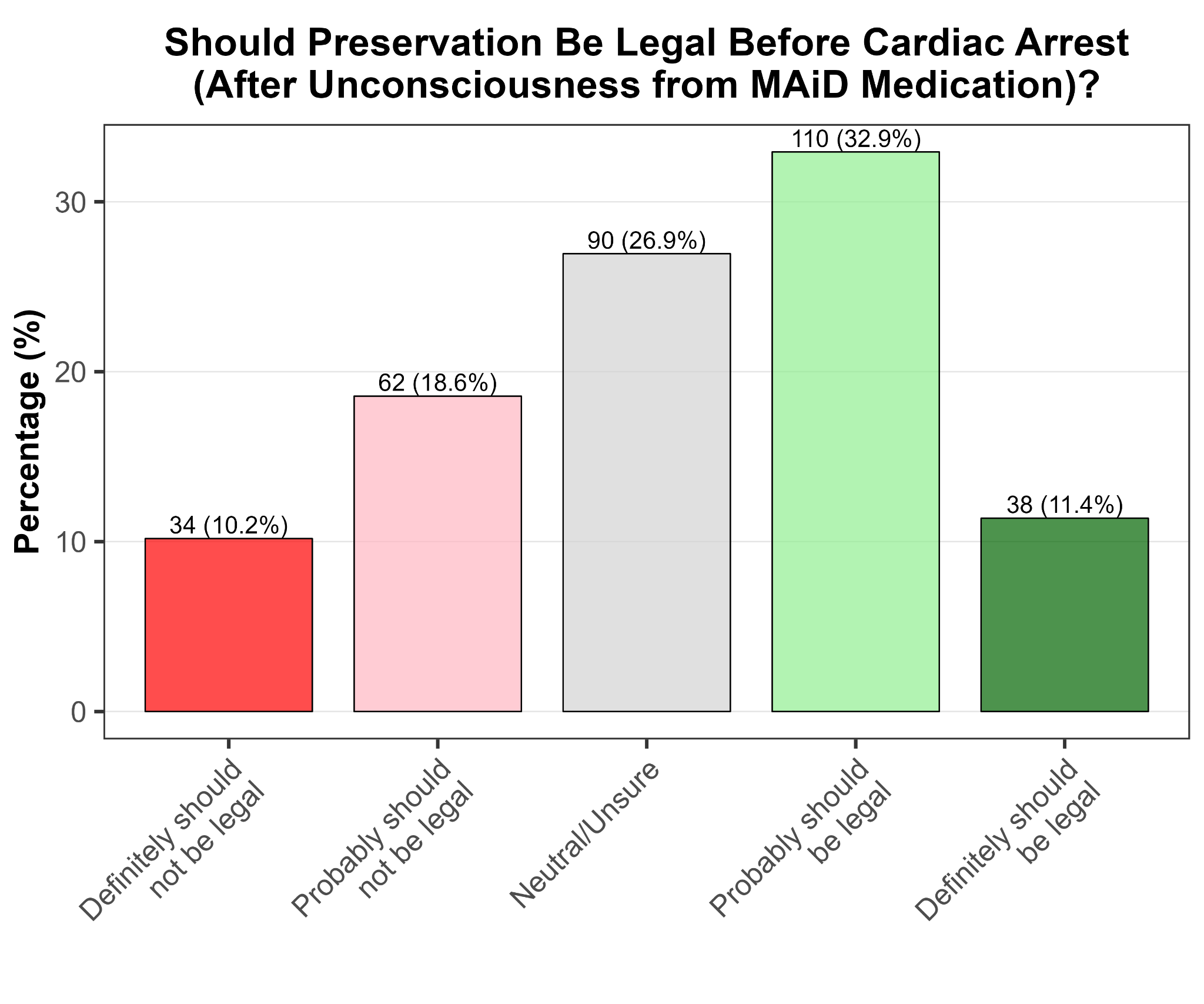
44.3% of respondents said this should probably or definitely be legal, while 28.8% said it probably or definitely shouldn’t be.
It’s still the case that more doctors support this intervention than oppose it, but it’s also clearly much more controversial than simply providing anticoagulants.
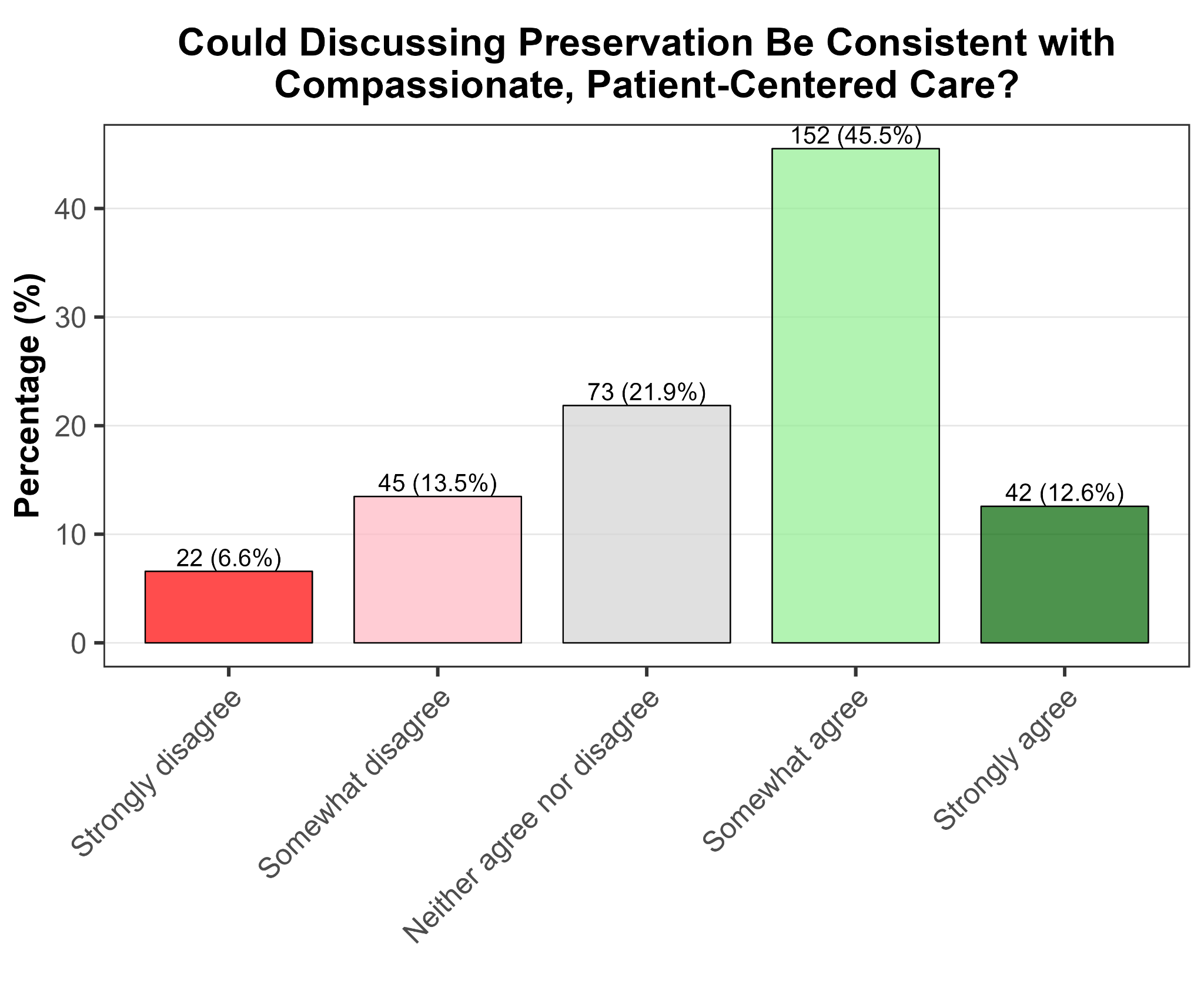
Beyond the question of whether preservation works, there’s the question of whether doctors are comfortable with it as a treatment option. Doctors are the gatekeepers to end-of-life care, and their attitudes matter enormously. Even if a physician thought preservation had a reasonable chance of working, their personal disdain for the procedure could make it functionally inaccessible to patients.
To determine this, we first asked whether doctors thought preservation could be compatible with compassionate, patient-centered care. We found 58.1% agreed, while only 20.1% disagreed.
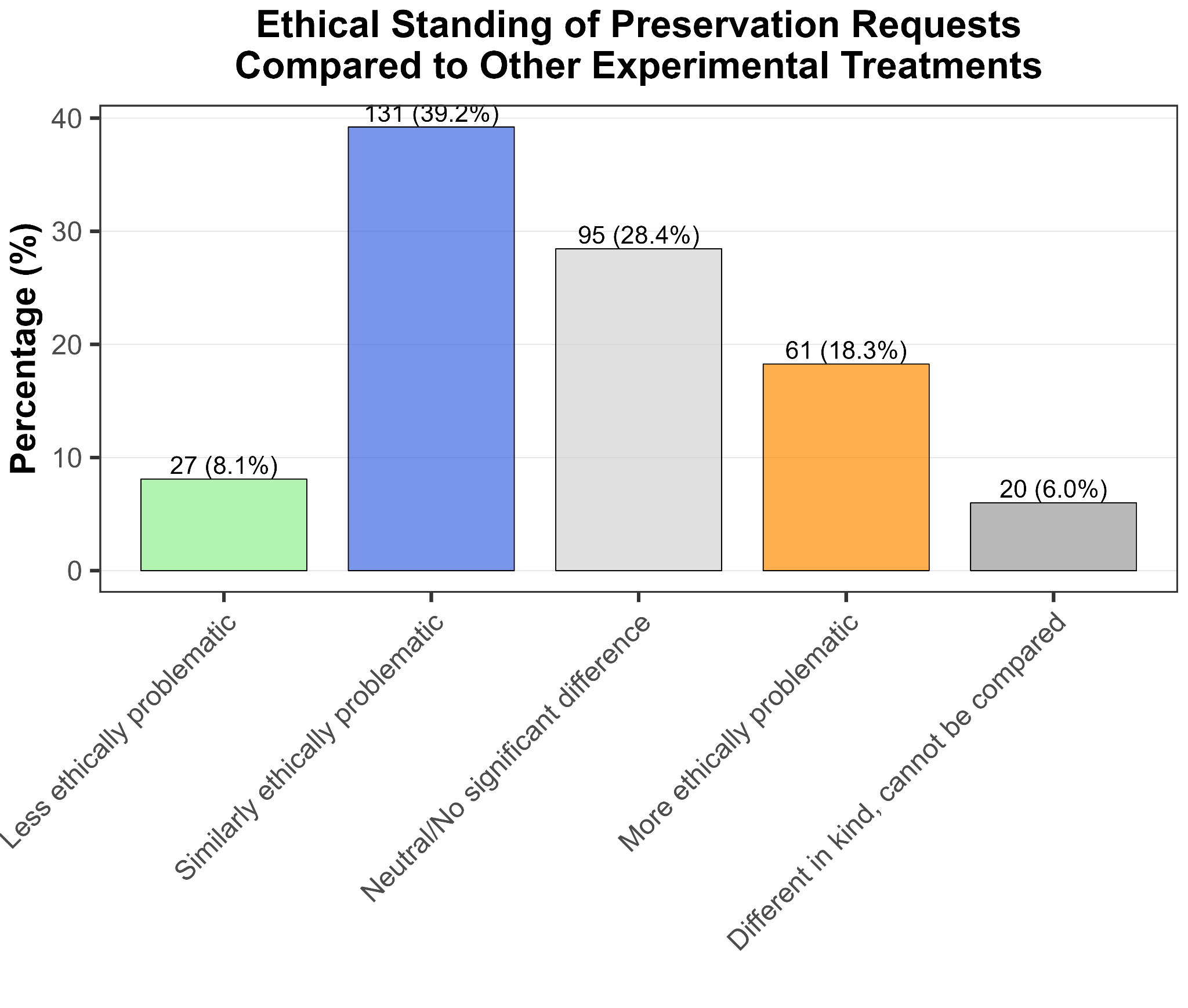
Next, we asked whether doctors saw preservation as ethically distinct from other last-ditch experimental treatments. For context, patients with cancers that are unresponsive to treatment can sometimes access unproven drugs through means like the Expanded Access programs in the US or the Early Access to Medicines Scheme in the UK. Preservation occupies similar conceptual territory: an unproven intervention for someone who has run out of validated options.
Did doctors agree with the philosophical parallels? We found 75.7% said preservation was either similarly or less ethically problematic than other experimental access schemes, with only 18.3% thinking it was worse.
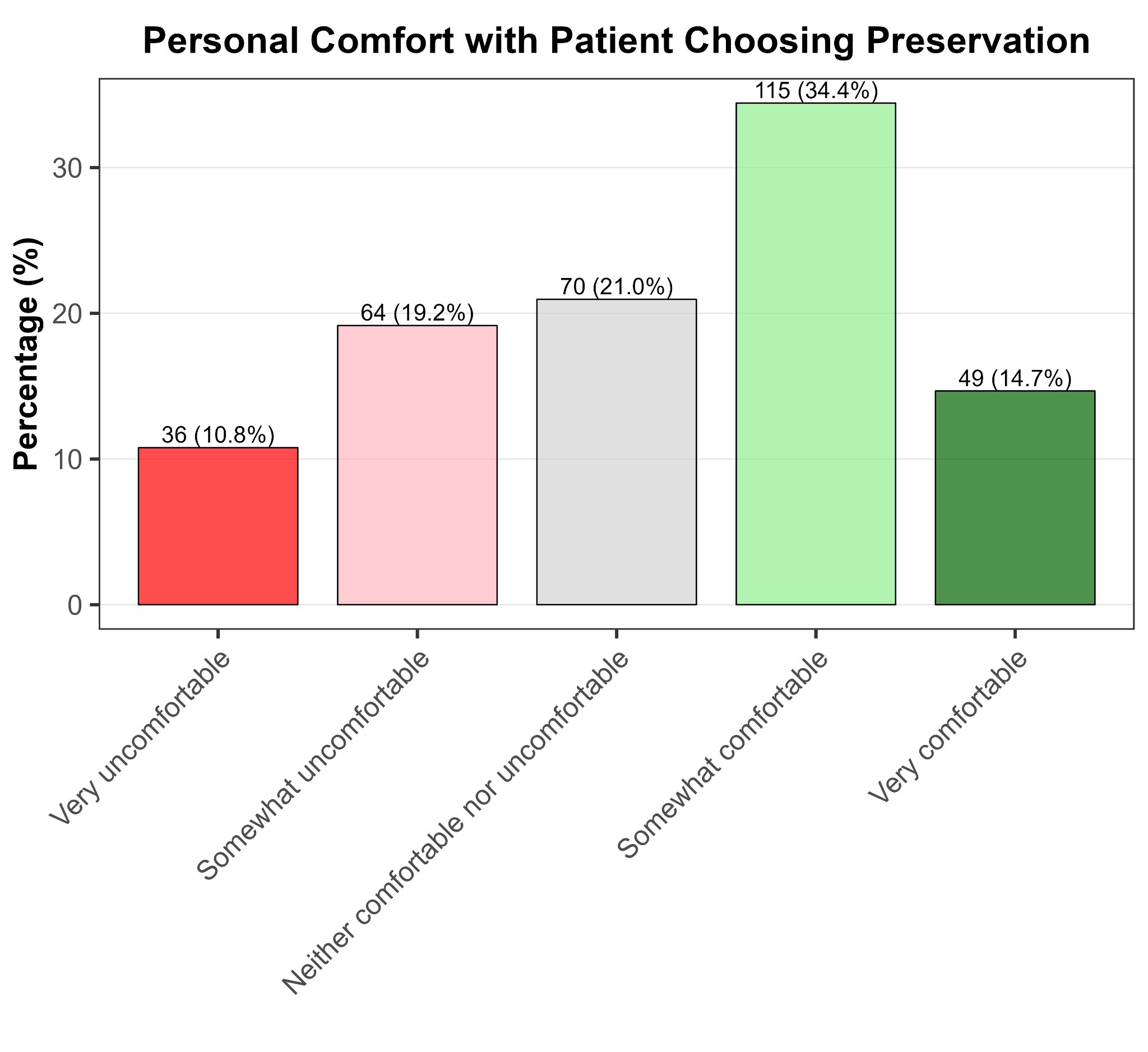
Lastly, when it came to their personal comfort with patients choosing preservation, 49.1% of doctors stated they were somewhat or very comfortable with it, while 30% said they were somewhat or very uncomfortable. Not exactly a ringing endorsement, but also not the wall of opposition that critics sometimes assume exists.
So what should we make of this?
First, the headline finding: the typical American doctor assigns a 25% probability to preservation eventually enabling revival, under ideal conditions.
That’s admittedly lower than the 40% the neuroscientists assigned to preservation retaining memories, but that makes sense - the scientists weren’t being directly asked about revival, just about memory retention and the possibility of using preserved brains to possibly create emulations (i.e. uploading).
Still, 25% is not a negligible number. Doctors routinely perform interventions with comparable or worse odds. About 22% of patients receiving CPR for out-of-hospital cardiac arrest survive to hospital admission; emergency resuscitative thoracotomy has a survival-to-discharge rate of around 8%; and salvage therapy for refractory leukemia has a one-year survival rate of under 26%.
Obviously we should be cautious here - comparing theoretical estimates to empirical survival rates is a bit apples-to-oranges. But the point stands: doctors regularly make use of treatments that have a 25% or lower chance of success, or support patients to access unproven experimental drugs with even lower odds. If preservation genuinely has these odds, it would not be unusual for doctors to support patients who wish to choose it.
And indeed, the results imply that in principle, most doctors would. The majority think preservation is compatible with compassionate care. The majority would accept pre-mortem anticoagulation to improve outcomes. A plurality would accept beginning preservation before cardiac arrest in MAiD cases. Whatever opposition exists to preservation, it isn’t coming from some unified wall of medical scepticism.
For patients considering preservation, this should be somewhat reassuring - your doctor is more likely to be sympathetic than hostile. For policymakers and legislators, these findings suggest that doctors would benefit from clearer frameworks that would let them support patients who request it. And for preservation advocates and organisations, this is evidence that the medical mainstream is potentially more open to engagement than you might have previously thought.
I’m obviously not a dispassionate scientist here. I want brain preservation for life extension to work. I want mainstream science and medicine to embrace the possibility that it might work. These results were not wholly dismissive of preservation, and as such, were the kind of results I was hoping for.
That’s worth being explicit about, because motivated reasoning is real. When scientists want a particular outcome - because they’re being paid to see or not see something, because the cause they believe in relies on certain results, because they need a positive result to publish so they can keep their job - they’re more likely to find it.
To combat this, we’ve tried to follow good open-science practices: the survey questions and raw participant response data are here for anyone to scrutinise. If you think we’ve made an error, or phrased our questions in leading ways, or cherry-picked our results, you have everything you need to check.
But what I’d genuinely welcome is replication. Maybe there’s something unusual about the Sermo platform that attracts unrepresentatively optimistic doctors, or maybe optimistic doctors are more likely to respond to surveys. Maybe American physicians differ dramatically from those elsewhere. Maybe our question wording was biased. If you’re sceptical, don’t just critique - run the study again and show me I’m wrong.
My prediction is that these results will hold up. And my guess is that if we repeat this survey in five or ten years, the numbers will be higher. As the neuroscience of memory solidifies, as preservation techniques improve, and as the medical community becomes more familiar with the idea, I expect the case for preserving the dying for a shot at revival will only grow stronger.