Make the case for preserving the brains of the dying, as I do, and one objection turns up without fail. I don’t mean the philosophical ones - whether a revived person would still be you, whether anyone in the future will bother reviving them - though those come up too. I mean the one about the money. “Isn’t this absurdly expensive? Isn’t it just a plaything for billionaires who can’t accept that they’ll die like the rest of us?”
The honest start to a response is to admit that yes, right now, if you’re paying out of your own pocket, it’s expensive. Sparks Brain Preservation charges around $100,0001, Tomorrow Biostasis wants about $228,000, and Nectome lists $250,000. So a shot at not dying currently runs somewhere between one and two-hundred-and-fifty thousand dollars.
That’s a lot of money. It should be much cheaper, and it saddens and disturbs me that it’s not. Even so, I’d argue, it’s completely reasonable by the standards of existing medical spending in the developed world.
First, those prices aren’t what the procedure itself costs; they’re what it costs to run a tiny operation for a few dozen customers a year while inventing an entire medical field as you go. The actual procedural work - clearing the blood, perfusing a chemical fixative, swapping the body’s water for a cryoprotectant so it can be cooled without ice tearing it apart - uses cheap, industrially-produced chemicals and a day of skilled labor. Done in higher volume, I’ve calculated the marginal cost at closer to $13,000, with storage on the order of a thousand dollars a year. Like every new technology, I expect the price to fall as it scales.
Second, what actually decides whether $150,000 is a bargain or a rip-off is the chance the procedure works. If that chance is zero, you’re just burning money. If it’s a certainty, then fork out whatever you’d spend to save your own life.
How likely is it to work? When we surveyed 334 American doctors last year and gave them an idealised case - an elderly patient preserved within minutes, brain structure confirmed intact down to the synapses - their median guess at the probability of eventual revival was 25%. Your number may be higher or lower, but let’s go with that.
If this were a normal calculation of expected costs and benefits, we’d multiply how much we’d be willing to pay for a guarantee of obtaining something by the probability that we actually receive it. There’s nothing exotic about that kind of sum: if I’d pay $30,000 to own a particular car outright, and you sell me a raffle ticket giving a one-in-ten chance of winning it, I shouldn’t hand over more than $3,000 for the ticket (the prize, marked down by the odds of actually getting my hands on it).
So feed preservation into the same calculation. Say the most a typical seventy-year-old would spend on a guaranteed return from death is half of everything they own. Median net worth for an American aged 65 to 74 is about $410,000, so call the guarantee worth $205,000. Mark that down by the 25% chance it works, and you arrive at roughly $50,000.
But applying this form of calculation to this situation feels absurd. What preservation buys, if it works, isn’t three more years, or ten - it’s an open-ended life, with no natural end date to cap the prize. Yet if you multiply a payoff that large by any probability above zero, you get something indistinguishable from infinity, and infinity times any non-zero probability is still more than everything you have. This is a Pascal’s mugging: a prize enormous enough that any probability, however microscopic, can justify any sacrifice, however ruinous. Almost no one can actually live this way, so let’s drop the multiplication.
Instead, let’s flip it around - what expensive medical services do individuals or healthcare systems already pay for, and how does preservation look sitting next to them? Instead of allowing theoretical calculations to push us in absurd directions, we can center ourselves through comparisons to therapies that are already deemed worthwhile.
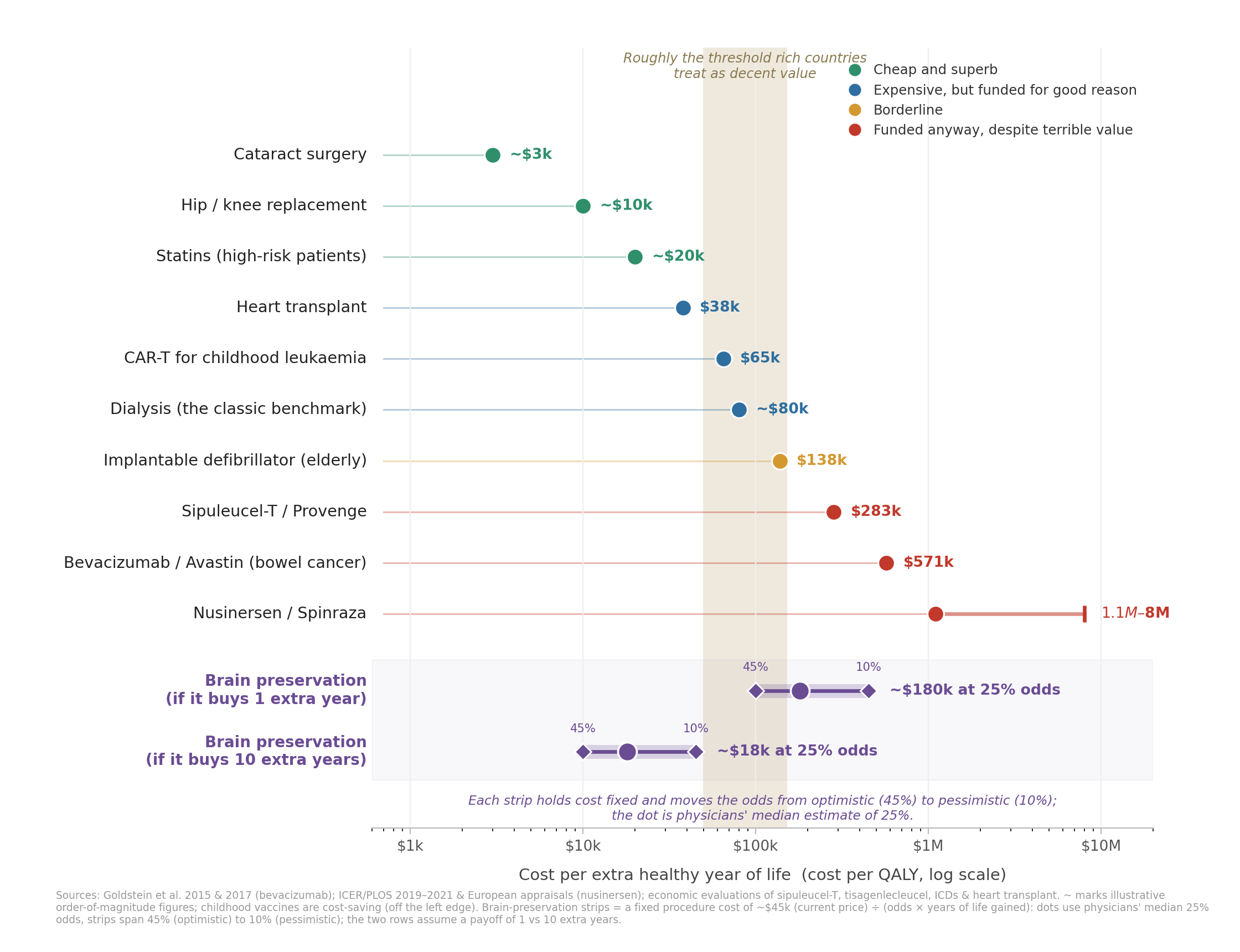
A final note before starting: the unit for this comparison is the cost per quality-adjusted life year: roughly, dollars per extra year of healthy life. Rich countries mostly treat anything under $50,000 to $150,000 per healthy year as decent value (Britain’s threshold sits a bit lower, the US is a bit higher and vaguer on theirs).
It’s easy to forget that much of medicine is cheap and superb. Childhood vaccines pay for themselves more than ten times over. Cataract surgery hands back a person’s eyesight for a couple of thousand dollars per year of vision restored. Hip and knee replacements, statins for the high-risk, drugs that help people quit smoking - all come in at a few thousand dollars per healthy year or less. This is what we want all of medicine to look like.
Some of medicine is expensive yet still worth every cent. A heart transplant runs to around $160,000 once you count the first year of care. Even so, healthcare systems will pay for this - despite one-in-ten recipients dying within the first year, and one-in-three by five years - because the survivors typically get nine more years, which works out to about $38,000 per year of life. CAR T-cell therapy - a treatment that can pull a child with otherwise incurable leukaemia into permanent remission - can cost over $400,000 per treatment. Yet in children, it can still land well under $100,000 per healthy year, because when it works it may well give back decades. These cases show we’ll spend real money, despite significant odds of failure, when the prize is enough life.
Then there’s the medicine that costs a fortune, barely works, and gets done anyway.
Take sipuleucel-T (Provenge), an immunotherapy for advanced prostate cancer. It costs around $100,000 and extends life by a median of about four months. That’s somewhere between $300,000 and $550,000 per year of life. It is a guideline-recommended, FDA-approved treatment option.
Or bevacizumab (Avastin), given as first-line treatment for metastatic bowel cancer. A 2015 US cost-effectiveness analysis found that adding it to chemotherapy bought about a tenth of a quality-adjusted life year - roughly six weeks - at around $570,000 per healthy year. A 2017 study extended the model to the UK, Canada, Australia and Israel. Local prices were lower, so the figure fell to somewhere between about $280,000 and $360,000 per healthy year, but the probability of clearing even a generous $150,000 threshold was zero in every one of them. It was adopted anyway: England’s NHS paid for it through the Cancer Drugs Fund, a pot created specifically to buy cancer drugs that were otherwise judged too poor value for routine use; while Australia listed it on its public subsidies scheme after first rejecting it on cost-effectiveness grounds.
A few more quick hits: Arthroscopic knee surgery for osteoarthritis has less than a one-in-five chance of being cost-effective even at the lenient $50,000 threshold, and it’s done hundreds of thousands of times a year across the US, Canada, and UK. Implantable defibrillators run past $138,000 per healthy year in the elderly and around $280,000 in some children, while evidence on their cost-effectiveness is mixed. Nusinersen (Spinraza), for spinal muscular atrophy, has been costed at $1.1 million per healthy year at best and $8 million at worst - figures that miss every threshold anyone has ever drawn by a factor of ten or more - and it’s funded by individuals, insurers, and public healthcare systems regardless.
To be fair, many of these treatments go to people who’ve exhausted every other proven option and are desperate for anything that might help. I have nothing but sympathy for them - it’s exactly the same sort of situation that those considering preservation are in. Still, the asymmetry is hard to swallow. When an oncologist reaches for a hundred-thousand-dollar drug that might win a patient a few more months, this is seen as perfectly understandable. Suggest spending that same money on a real, if uncertain, shot at an indefinite life, and some of the same people who would say the oncologist was “doing everything they could” would decry the expenditure as exorbitant and foolhardy.
If a one-in-four shot at indefinitely more years costs the same as some treatments already in routine use, where is the contempt coming from? My honest suspicion is that it has very little to do with the money at all.
Consider what happens when you take the cost away. For a stretch, Sparks offered its preservation procedure for little to nothing. A number of the people preserved by them and other organisations have paid a reduced fee or none at all, with financial aid on hand for those who couldn’t otherwise afford it. If the price were the sticking point, you’d expect some commentary on the alleviation of this objection, but I’m not aware of any critics providing even a grudging acknowledgement.
Nor do I think that halving the sticker price would similarly halve the scorn, any more than I believe that nudging the experts’ credence from 25% up to 45% would move public opinion equivalently to match. Whatever the critics are doing, they are not sitting down, weighing costs against odds, and concluding that preservation isn’t worth it just yet - but might be once the evidence firms up or the price comes down.
Instead, I think they’re looking at a practice that seems weird and distasteful, dismissing it on that basis, and reaching for the price tag afterwards to make the dismissal sound rigorous. This is made all the easier when the field in question has a history of acting outside the scientific and medical mainstream, avoiding rigorous evaluation of its own methods, and suffering the occasional organisational collapse or legal scandal.
So our job as advocates’ is to earn the credence we’re asking for - careful science, replicable results, avoiding overpromising, and making serious efforts to bring preservation inside the tent of ordinary medicine. But critics have a job too, which is to figure out what they actually object to. “It won’t work”, “it’s weird”, and “it’s too expensive” are three entirely separate arguments, each standing or falling independently. Pull them apart, say which one you’re really making, and evaluate each on its own merits instead of bundling them together.
It’s not that there aren’t valid objections to be made. Preservation is still too expensive today (even if it’s a price worth paying). No group has yet preserved a human being to the standard that won the Brain Preservation Prize in a laboratory setting, let alone shown it can do so reliably in a real clinical setting. Even so, I expect the methods will improve over time, much as the costs should fall the way they always do once a practice stops being bespoke.
But critics should remember we live in a world that spends fortunes on medicines of middling value - cancer drugs that buy weeks-to-months, million-dollar-a-year orphan drug treatments - and does it without apology. The United States goes further and legally bars its own federal health programs from formally weighing cost against benefit at all, precisely so that nobody has to say out loud what a year of life is worth. In a system that squeamish about pricing life, and that generous towards treatments that barely work, the real absurdity is singling out as too expensive the one intervention that might, if it works, hand back all the years there are.