Are We Waiting Too Long to Treat Adolescent Idiopathic Scoliosis? That is the 20 degree question.
For decades, parents have been told the same thing:
“If the curve is around 20°, we watch.”
It sounds reasonable. Conservative. Safe.
But what if that threshold—20° Cobb—is not a safe place to wait?
What if it is the point where the spine begins to change in a way that becomes harder to reverse?
One of the most important things to understand about scoliosis is this:
The spine is not just a stack of bones.
It is a living system.
Bones grow
Discs adapt
Ligaments respond
Muscles compensate
And most importantly:
The spine learns.
When a curve develops, the body doesn’t simply tolerate it—it begins to adapt to it
.
At first, scoliosis may be flexible.
The spine can still correct. The tissues are still responsive.
But as curves approach the 20° range, three key processes begin to accelerate:
The disc is the “cushion” between the bones of the spine.
In a healthy spine, it distributes load evenly—like a water-filled balloon.
But as curvature increases:
Pressure becomes uneven
The soft center of the disc shifts
The outer ring is stressed asymmetrically
Over time, the disc becomes wedge-shaped.
This is critical.
Because once that happens:
The disc is no longer just responding to the curve—it begins to drive it.
And unlike bone, discs have very limited ability to remodel back to normal.
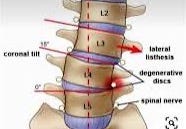
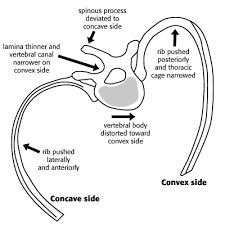
Scoliosis is not just a side-to-side curve.
It is a three-dimensional deformity involving:
Lateral bending
Vertebral rotation
Rib cage distortion
As rotation progresses:
Forces across the spine become increasingly uneven
Growth plates experience asymmetric loading
The deformity reinforces itself
This creates a feedback loop:
Rotation → asymmetric load → more rotatio
n
Over time, the body adapts to abnormal forces. Just think of orthodontic braces on teeth. Time can do wondrous things.
Vertebral bodies begin to wedge
Discs remodel
Ligaments stiffen
Soft tissues adapt
At this stage:
The curve is no longer just a posture—it becomes part of the structure.
And structural problems are far more difficult to correct than flexible ones.
If intervention occurs before these changes become established:
Discs remain symmetric
Rotation is limited
Vertebral bodies are still normal
In other words:
We are working with a system that can still respond.
This is a fundamentally different situation than treating a spine that has already remodeled.
Traditionally, treatment has been divided into two paths:
Observation
Fusion surgery
But this may be an oversimplification.
There is a third concept emerging:
Guiding the spine—rather than forcing it.
Biology tends to respond best to:
Gradual change
Controlled mechanical input
Time to adapt
This is why I have become increasingly interested in:
Gradual alignment strategies
Using systems that allow the spine to:
adjust slowly
adapt biologically
remodel toward a healthier state
Rather than forcing immediate rigid correction with larger deformities where inadvertent spinal cord stretching may occur.
.
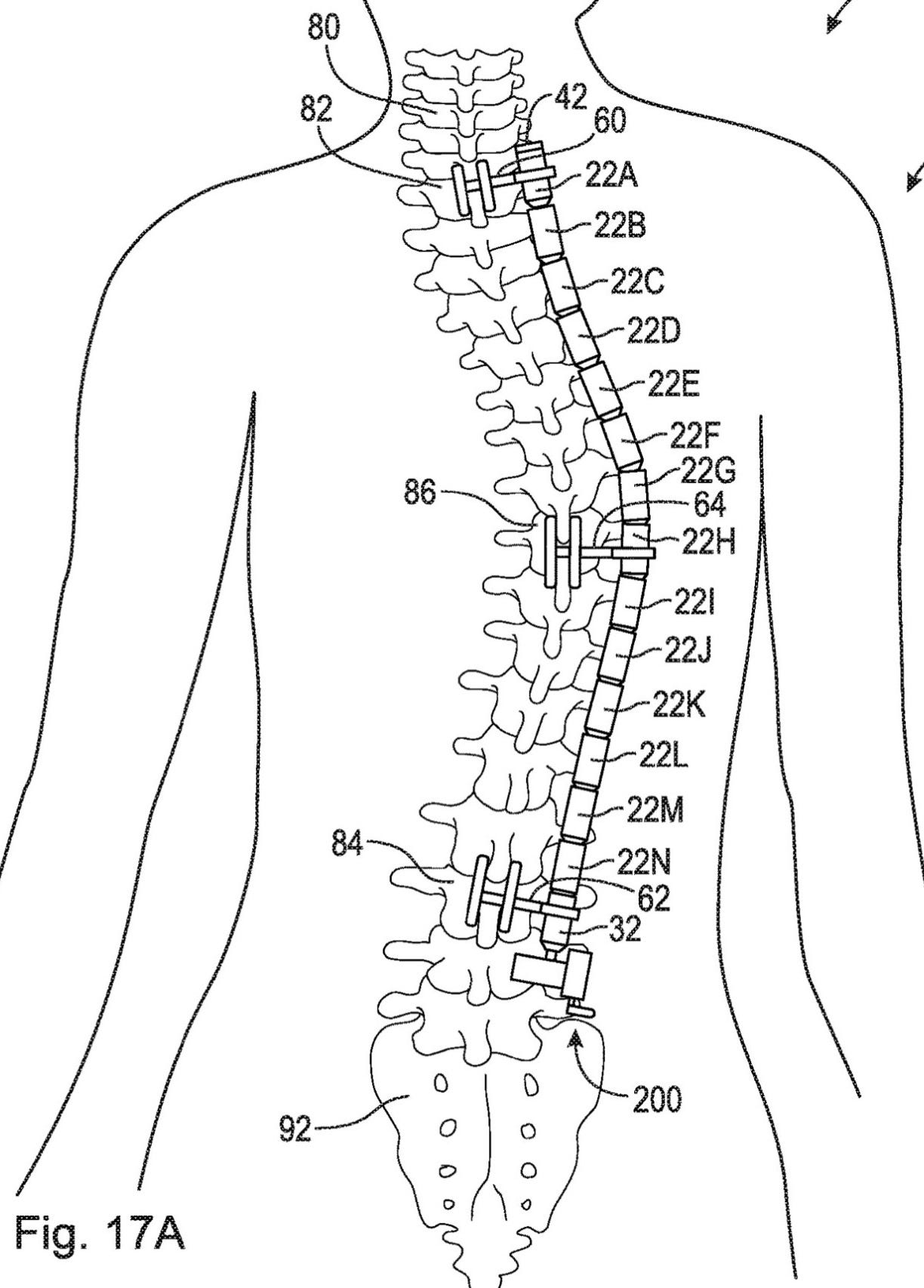
As the individual segments are drawn taut gradually, they nest into each other in a pre planned and pre fitted male/female fashion so the final shape is a perfect, customized S shaped spine with full coronal and sagittal balance. This is done before permanent changes occur in the disc. The device permits full mobility during alignment and may even be able to be removed without fusion once skeletal maturity is reached. If fusion is required, it could be done endoscopically at the apical pathologic vertebral level.
If your child has scoliosis, the most important question may not be:
“Will it progress?”
But rather:
“Has the spine started to remodel?”
Because once remodeling begins, the window for simpler, more biologically responsive treatment begins to narrow. Living with even a lesser ‘fixed’ curve is not necessarily a normal life. Malalignment stretches muscles and ligaments causing various degrees of discomfort. Sometimes even disabling pain.
Spine surgeons, parents, and patients alike may want to reflect on this:
Are we waiting for curves to get worse…
Or are we waiting for the spine to become harder to treat?
The goal is not simply to immobilize the spine.
It is to guide it.
To intervene while the biology is still responsive. To treat when the operation is much easier and safer. To treat when the spine is malleable and alignment force is minimal.