For several decades, the standard approach to autoimmune diseases has been suppression of the immune system, a treatment with potential serious side effects and, with the common use of injectable monoclonal antibodies, variable efficacy, at very high cost. For example, Humira (adalimumab), an antibody vs tumor necrosis factor used as treatment for many autoimmune diseases, has a list price of over $7,000 a month and was for a decade until 2022 the leading drug by sales worldwide (peak $22 billion of sales in 2021, before patent expirations). That ought to give you a sense for how prevalent autoimmune diseases are in the world. Notably, about 10% of the world’s population has an autoimmune disease. I have previously written in Ground Truths about the approximate doubling of risk of autoimmune diseases, across the board, after Covid.
But there is a remarkable pivot now that has accelerated in 2025 to achieving cures!
I wrote about this in a SUPER AGERS chapter entitled “ Controlling Our Immune System” and this approach is rapidly pushing forward. This edition of Ground Truths will cover: (1) the 2 major shots on goal for curing autoimmune diseases, and (2) how all the progress in immunotherapy for cancer is laying the foundation.
Let’s first run through the 2 major potential routes to cure.
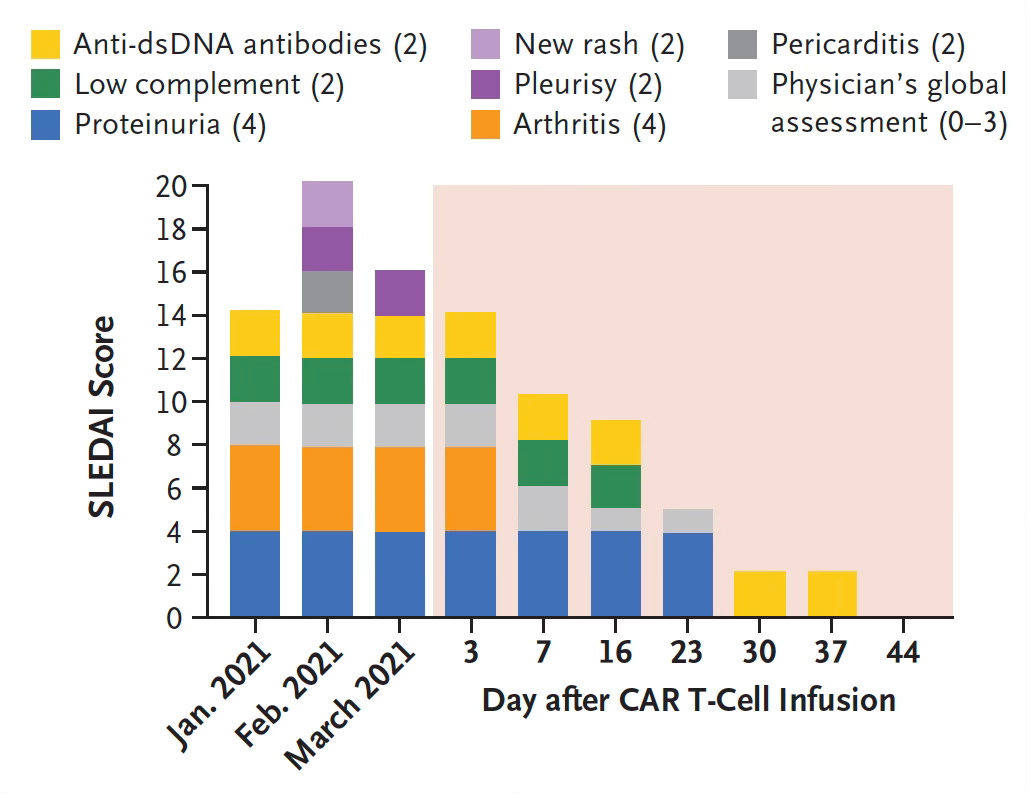
CAR T cells have been used for cancer with marked success for certain types of blood “liquid” cancers, but much less efficacy in solid tumors, an area of extensive ongoing research. In 2021 in Germany , a single infusion of CAR T cells targeting CD-19 led to the first cure of a 20-year-old woman with severe, refractory systemic lupus erythematosus (SLE). This was a dramatic case report, as exemplified by the Figure below. Look how all these conditions resolved over 6 weeks.
A few years later the same group of German researchers, led by Georg Schett, demonstrated more prolonged remission and cures for patients with lupus, systemic sclerosis and idiopathic inflammatory myositis. Such work has been extended to multiple sclerosis with the CD-19 target or, more recently, with a B cell maturation antigen that extends the target to long-lived plasma cells (and dual targeting CARs vs CD19 and BCMA). The work for CAR T in autoimmune disease has been assessed for many other diseases including myasthenia gravis, stiff person syndrome, ,neuromyelitis optica spectrum disorder, pemphigus vulgaris, rheumatoid arthritis, Sjogern’s disease, and Type 1 (autoimmune) diabetes. Systemic sclerosis has been successfully approached with CAR NK, engineered cells directed against natural killer cells. Some of these diseases have been using other targets besides CD-19, such as CAR-Treg (regulatory T cells that put on the brakes of the immune system, their discovery won the Nobel prize in 2025) for rheumatoid arthritis and type 1 diabetes or an antigen-specific B cell receptor (DSG3-CAART) for pemphigus, a life-threatening skin disease caused by autoantibodies vs desmoglein (Dsg3).
Why is this referred to as a “Hard Reset”? It’s because the B cells are depleted and when they repopulated there’s no longer the self-attacking, disease-causing immune cells. It is as if the new, naive lymphocytes forgot they were previously engaged in warfare, a veritable resetting of the immune system. Like rebooting your computer the was not working and then everything runs fine..
But until 2025 the CAR T field relied on outside the body (ex vivo) engineering of the T cells. That’s laborious, time consuming, with complex manufacturing, very expensive, requiring hospitalization and chemotherapy. It requires all of a person’s lymphocytes to be removed and transferred to a facility where the cell engineering can be done, and a ~3-week delay for the CAR T infusion.
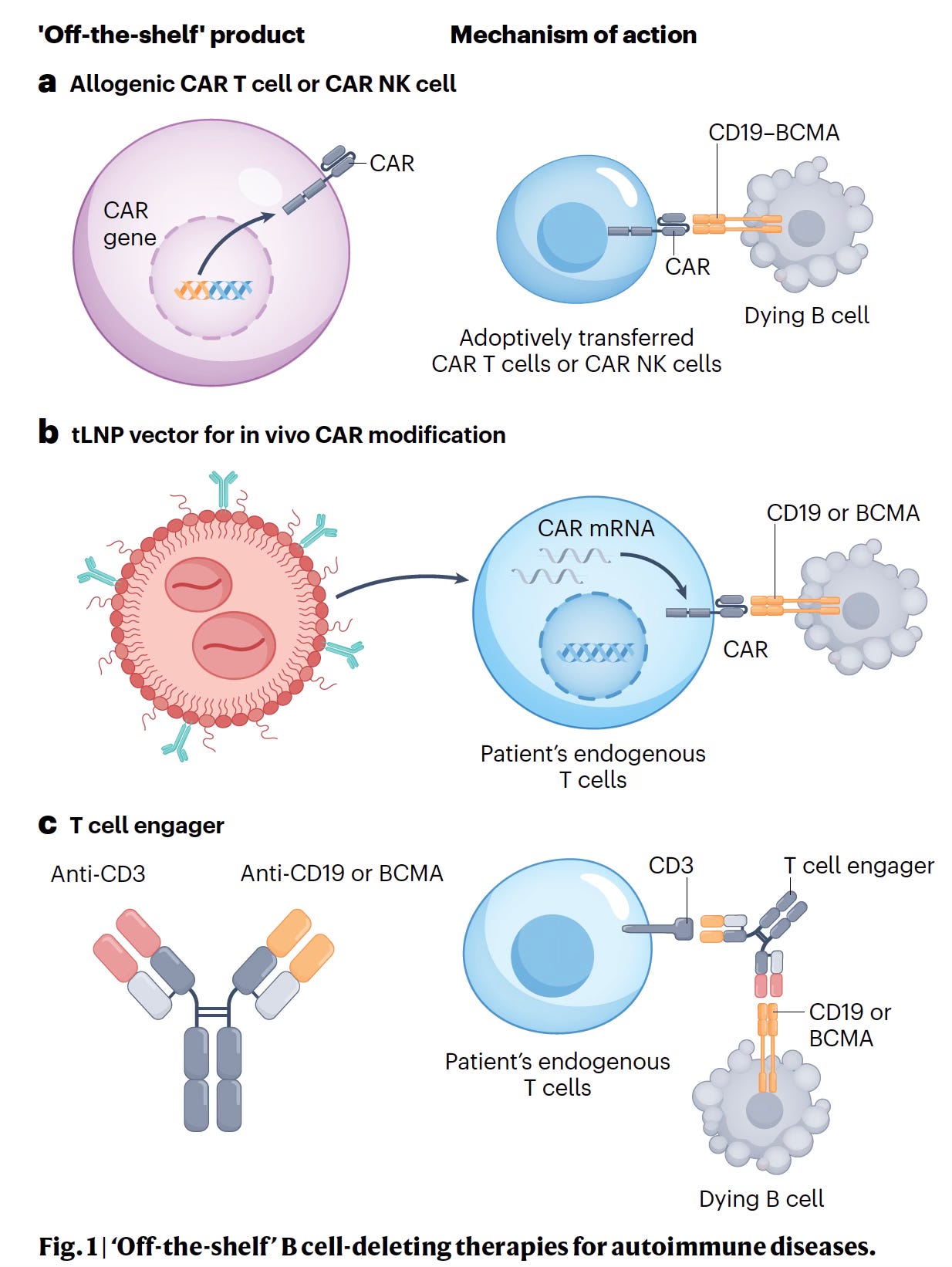
Now everything is moving toward off-the-shelf, universal, inside the body (in vivo), known as allogeneic, from healthy donors or a master cell bank, with the key requirement of a delivery mechanism such as a lentiviral vector or mRNA with lipid nanoparticles (LNP, panel b) or bispecific antibody (panel c below) that pairs up the T and B cell it’s meant to kill. The latter achieved lasting remission with deep B cell depletion in 6 of 10 patients with refractory autoimmune diseases but is transient as compared with the lentivirus vector or mRNA delivery durable approaches. The in vivo, in-the-body strategy avoids the need for lymphocyte depletion that requires chemotherapy with its attendant toxicity. This can be done as an out-patient, preempting a prolonged hospitalization for a patient waiting without lymphocytes, and preserving the patient’s immune system.
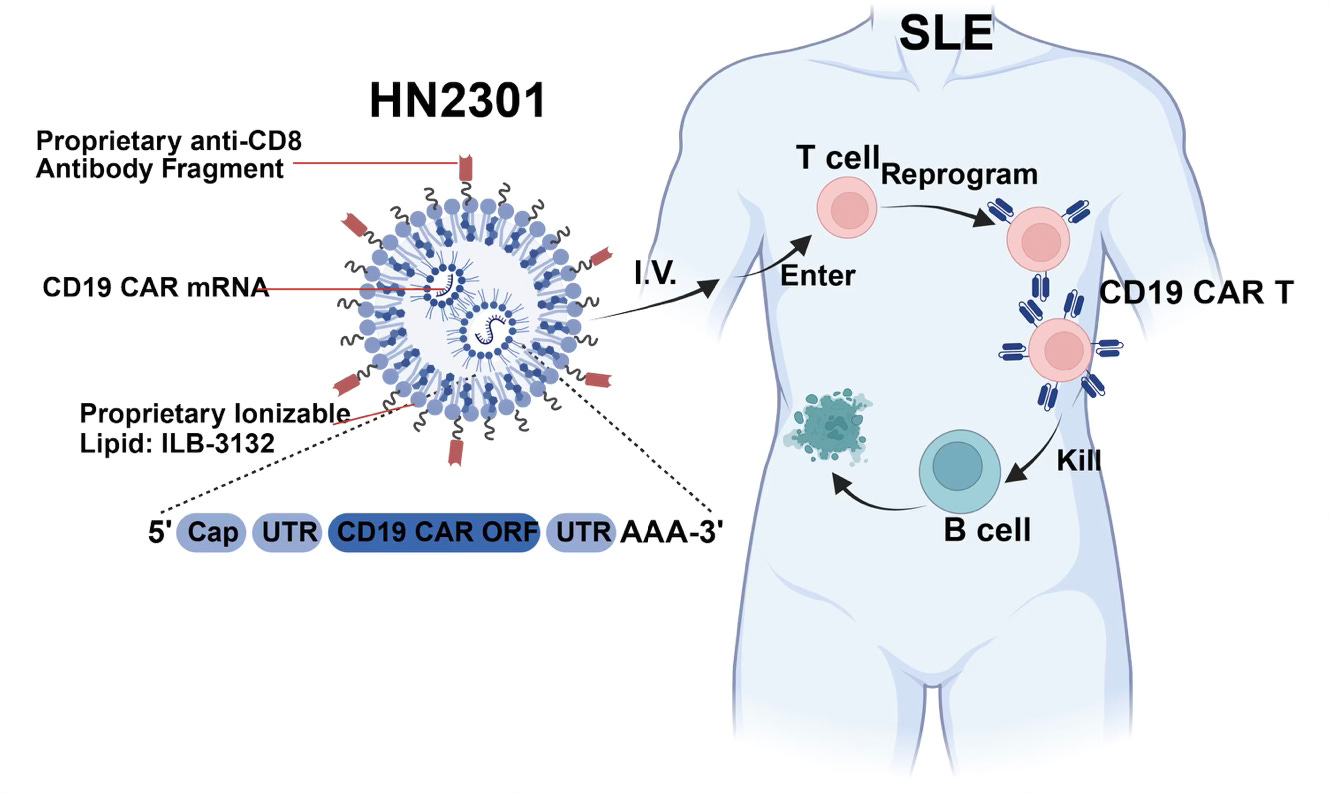
This inside the body, off-the-shelf strategy has already been shown to be safe and successful in Phase 1 trials of refractory SLE and in patients with systemic sclerosis or severe myositis. Below is a schematic from a recent report of 5 cases with success for SLE in vivo using mRNA for delivery; HN2301 is an engineered lipid nanoparticle.
Several companies are in clinical trials with in vivo CAR T for autoimmune diseases including Capstan Therapeutics, Kite Therapeutics, Umoja Biopharma, and Shenzhen Magic-RNA. The striking progress in this field towards universal, potential one-shot cures is tempered by residual anticipated high cost, the cytokine release syndrome and neurotoxicity that can occur with CAR T. The mRNA and non-viral vectors are considered a better choice than a lentivirus vector because of the latter’s potential risk of mutagenesis and cancer.
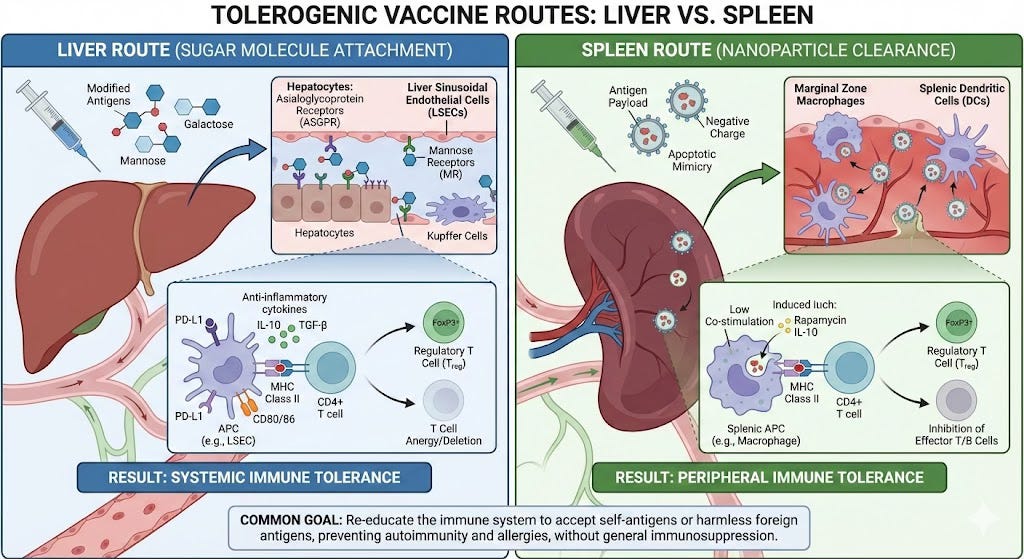
I wrote about this in a prior Ground Truths on tolerogenic vaccines, the opposite of standard vaccines that boost the immune system. By leveraging the liver, an immune-privileged organ that when processing an antigen target, by attaching with a sugar, the liver can flag it as safe and issue a “do not attack.” Alternatively, tolerance can be achieved via the spleen route by masquerading the target antigen inside lipid nanoparticles. Inverse vaccines are being pursued in celiac disease (Anokion, with positive clinical trial results reported earlier this year) , multiple sclerosis (Anokion, Moderna, BioNTech), and Type 1 diabetes (Diamyd Medical), rheumatoid arthritis (Janssen) clinical trials.
With the help of Nano Banana I made the infographic below to demonstrate the two mechanisms (of many) to achieve tolerance with vaccines. Other non-vaccine, cell therapy routes include use of Tregs (such as via CAR-Tregs) that put the brakes on the immune system or dendritic cells that have been transformed to be tolerogenic. I won’t go into the details here but this recent review paper provides that information, with new methods to produce abundant, long lasting T regs. Notably, the mechanism by which dendritic cells can achieve immune tolerance was just published this week.
The other potential longer term strategy I want to call out is thymus rejuvenation. The thymus glad involutes in adolescence and many autoimmune diseases are age-related. We recently have learned much more about the thymus gland’s biology, evolution, and how given FGF21 can restore function of the involuted thymus. Also, just last week there was a publication on the molecular mechanism for how axolotl, a vertebrate, is able to regenerate its thymus gland from scratch after it has been removed. All of this could be useful for either prevention or potential cure of some autoimmune diseases in the future.
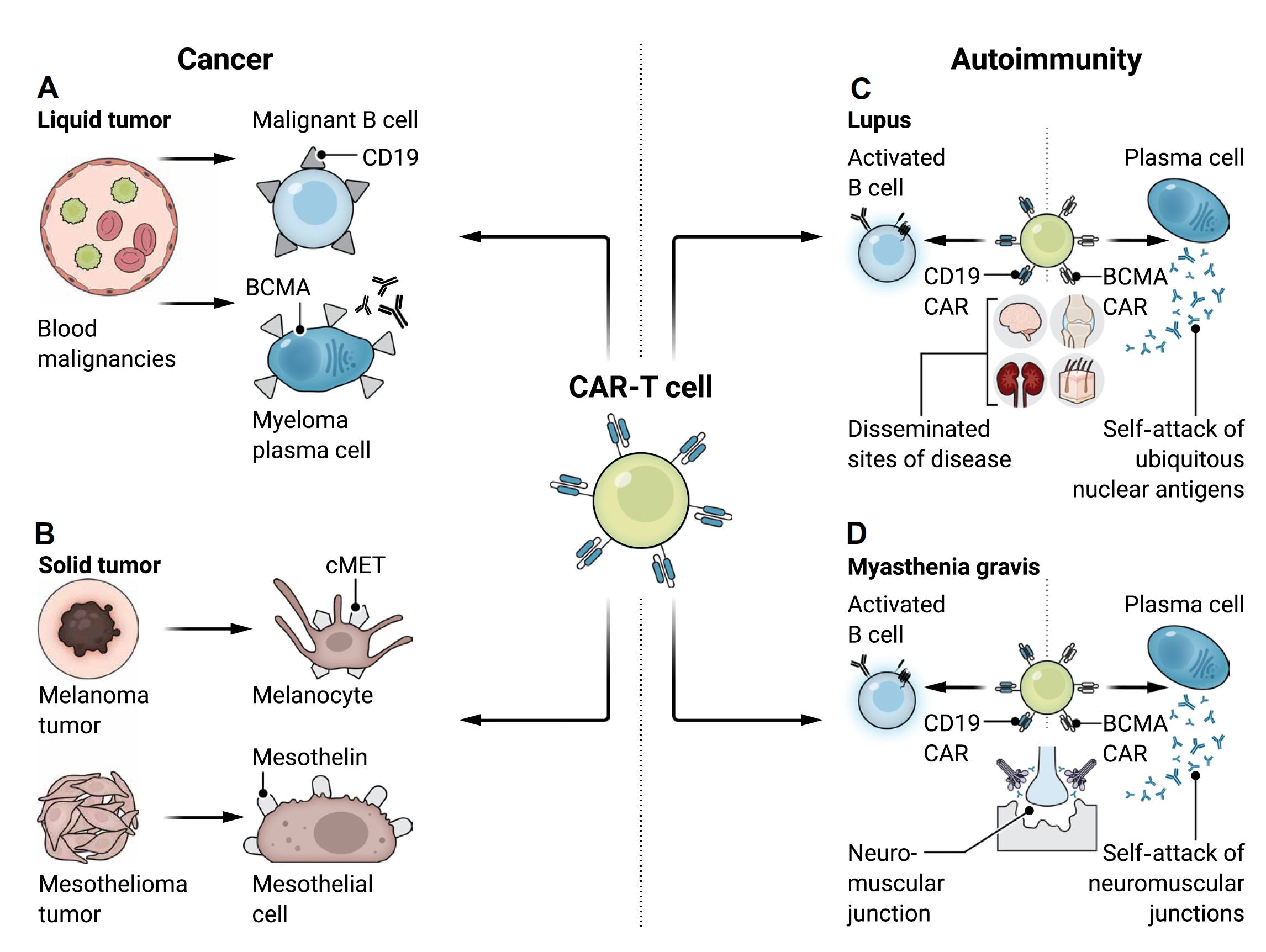
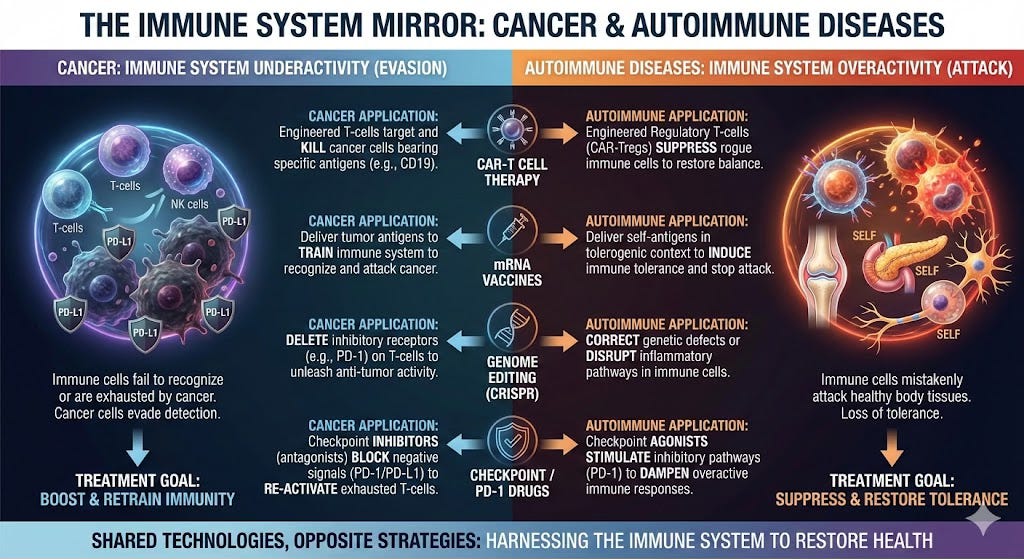
Cancer biology is the mirror image of autoimmunity. Predisposition to cancer occurs when the immune system is hypoactive, losing its protection, whereas autoimmune disease reflects hyperactivity and a dysregulated state. The approach to these 2 different diseases is like a rheostat, dialing the immune system up for cancer or down for autoimmune disease. The B cells are a common culprit, hence the successful use of CAR T vs B cells for both diseases. The checkpoint inhibitor PD-1 (prototype Keytruda) is to cancer (cut the brakes on the immune system) as PD-1 agonists (slam on the brakes) are to autoimmune diseases. Similarly, cancer vaccines to rev up immunotherapy are the opposite of inverse, tolerogenic vaccines as reviewed above. CRISPR genome T cell editing could amp up T cell killing function for cancer or make them into T-reg peacekeepers to stop autoimmune attacks. This review paper and its Figure below demonstrates the reciprocal relationship between CAR T for cancer and autoimmunity. What is important to emphasize is all the work to achieve in vivo, universal CAR T works for both diseases. Anything that helps cancer immunotherapy has the big dividend of also helping the efforts for curing autoimmune diseases. The new field of structural immunotherapeutics has legs to achieve precise control of our immune system vs either sets of diseases.
I’ve been impressed with the output from Gemini-3 Nano Banana for making science infographics, so I made this one for the mirror images of these 2 diseases.
I hope I am able to adequately convey the excitement in this field. This represents one of the biggest shifts in a domain of medicine that we’ve seen in decades. It has been stunning to see for the first time one-shot cures in patients who were refractory to all approved treatments. There’s a paucity of true cures in medicine. Considering that 1 in 10 people have an autoimmune disease, and these conditions have never garnered the level of attention as cancer, cardiovascular, or neurodegenerative diseases, these big steps of progress are especially welcome. Mirror biology and goals of all the clinical work in cancer directly benefits autoimmune diseases, turbocharging this movement.
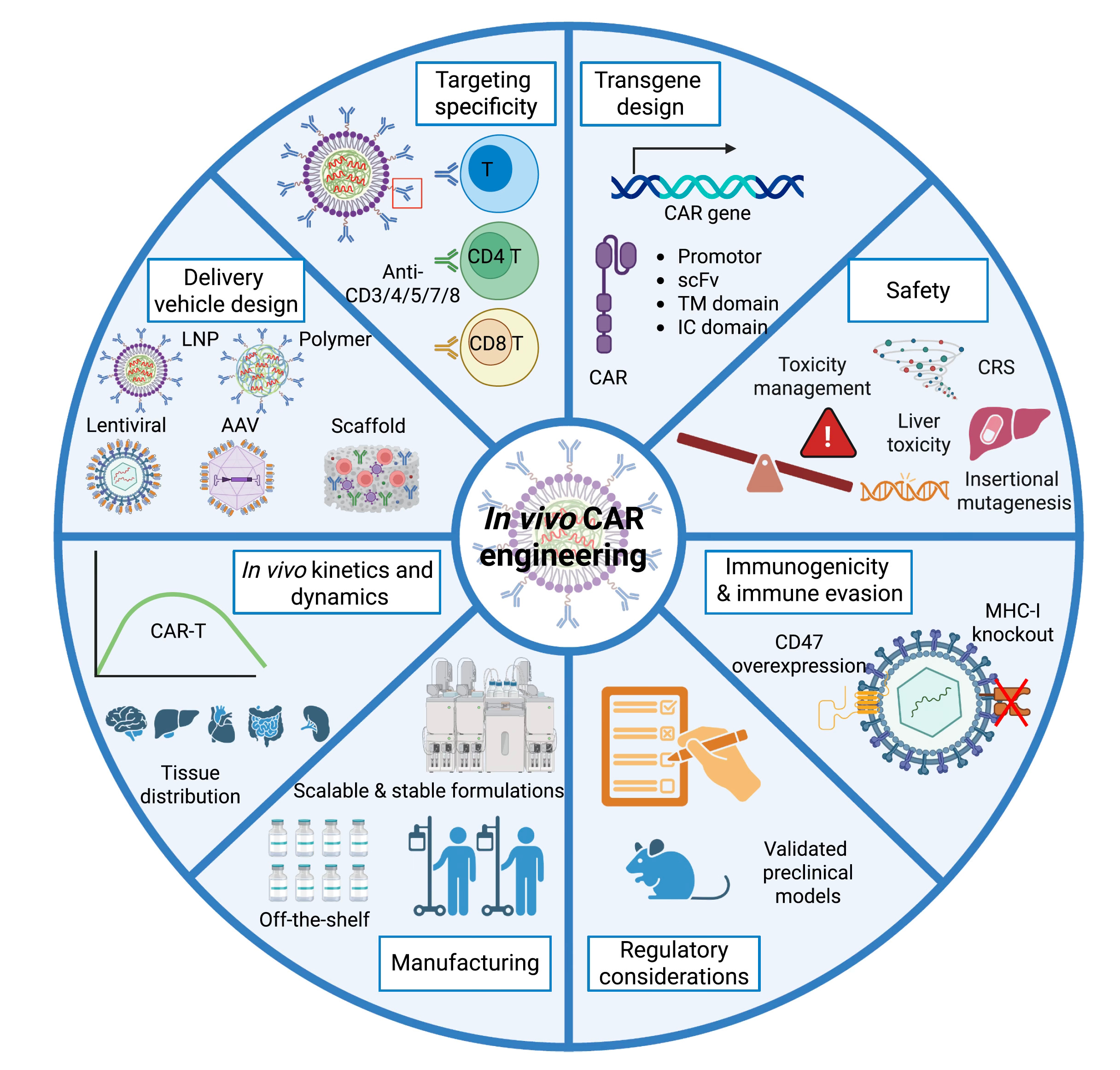
It’s still early, but most major autoimmune diseases are getting approached by both engineered cells and inverse, tolerogenic vaccines. The off-the-shelf, universal engineered cell approach is ahead of the inverse vaccines so far, and the refinements in the works are extensive, as shown in the Figure below. Eventually, both major routes of cell therapy and tolerogenicity are very likely to pan out and we should see a big dent in autoimmune diseases in the future. Of course, for any scaling, this will require availability at low cost, limiting side effects, making in practical and accessibility to all, avoiding inequities. But given all the rapid progress I’m confident we’ll get there in the years ahead. We’e seeing the initial stages of a renaissance vs autoimmunity. Curing instead of just treating autoimmune diseases.
Last week, I did the Big Interview at WIRED on the science of super agers and extension of our healthspan. You can view it here, with transcript

Also on a related immune system disorder, Long Covid, this week we finished enrollment for the 1,000 participants randomized to tirzepatide vs placebo, the first large RCT for this debilitating condition affecting millions of people with no known validated treatment.
I’ll be interviewing Dan Buettner on Blue Zones tomorrow, 15 Dec, live on Ground Truths at 12:30 PM. And later this week 17 Dec, with Dr. Jonathan Kipnis on getting toxic waste products out of our brain. Join us via the app. *****************************
Thanks to >190,000 Ground Truths subscribers from every US state and 210 countries. Your subscription to these free essays and podcasts makes my work in putting them together worthwhile.

If you found this interesting PLEASE share it!
Paid subscriptions are voluntary and all proceeds from them go to support Scripps Research. They do allow for posting comments and questions, which I do my best to respond to. Please don’t hesitate to post comments and give me feedback. Let me know topics that you would like to see covered.
Many thanks to those who have contributed—they have greatly helped fund our summer internship programs for the past two years. It enabled us to accept and support 47 summer interns in 2025! We aim to accept even more of the several thousand who will apply for summer 2026