Overview
Background
Cold agglutinin disease is a rare form of autoimmune hemolytic anemia caused by cold-reacting autoantibodies. [1] Autoantibodies that bind to the erythrocyte membrane and lead to premature erythrocyte destruction (hemolysis) characterize autoimmune hemolytic anemia. Peripheral blood smears may reveal clumps of red blood cells (RBCs). See the image below.
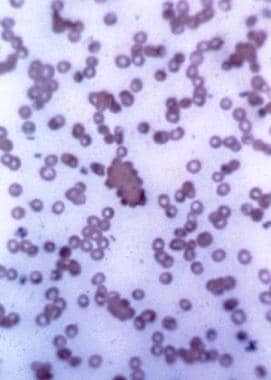
Peripheral blood smear showing several clumps of RBCs with the largest in the center. These are typical of aggregates seen in persons with cold agglutinin disease.
A common complaint among patients with cold agglutinin disease is painful fingers and toes with purplish discoloration associated with cold exposure. In chronic cold agglutinin disease, the patient is more symptomatic during the colder months.
Autoimmune hemolytic anemia is classified as primary or secondary and is subclassified according to autoantibody type. Primary cold agglutinin disease is characterized by a clonal lymphoproliferative disorder. [2, 3] Secondary cold agglutinin syndrome results from a systemic disease — infection or malignancy. [4]
In 90% of cases, the autoantibody in cold agglutinin disease is immunoglobulin M (IgM); rarely, it may involve monoclonal immunoglobulin G (IgG), immunoglobulin A (IgA), or λ light chain restriction. In contrast, warm autoimmune hemolytic anemia predominantly involves IgG. [2] Donath-Landsteiner hemolytic anemia is also caused by a cold-reacting immunoglobulin, but most cases are due to polyclonal IgG. [2]
Another autoimmune hemolytic anemia syndrome associated with cold-reacting autoantibodies is paroxysmal cold hemoglobinuria, which involves the IgG Donath-Landsteiner (D-L) antibody. Unlike cold agglutinin disease, in which affected RBCs are removed via extravascular phagocytosis, paroxysmal cold hemoglobinuria involves intravascular hemolysis. (See DDx.)
Primary and secondary disease
Primary cold agglutinin disease is usually associated with monoclonal cold-reacting autoantibodies. Primary cold agglutinin disease is chronic and occurs after the fifth decade of life, with a peak incidence in the seventh and eighth decades.
Secondary cold agglutinin disease may be associated with either monoclonal or polyclonal cold-reacting autoantibodies. It predominantly is caused by infection and lymphoproliferative disorders. Monoclonal secondary disease is usually chronic, occurring in adults. Polyclonal secondary cold agglutinin disease, which occurs in children and young adults, is usually transient.
![]()
Etiology
Cold agglutinins develop in more than 60% of patients with infectious mononucleosis, but hemolytic anemia is rare.
Classic chronic cold agglutinin disease is idiopathic, associated with symptoms and signs in relation to cold exposure. Causes of the monoclonal secondary disease include the following:
-
Nonhematologic neoplasms
Causes of polyclonal secondary cold agglutinin disease include the following:
-
Mycoplasma infections - M pneumoniae [6]
-
Infectious mononucleosis due to Epstein-Barr virus (EBV) or cytomegalovirus (CMV)
-
Other viral infections - Mumps, varicella, rubella, adenovirus, HIV, influenza, hepatitis C
-
Bacterial infections - Legionnaire disease, syphilis, listeriosis, Escherichia coli
-
Parasitic infections - Malaria, trypanosomiasis
Bacterial and viral infections
Transient acute hemolysis may occur secondary to certain infectious diseases, such as M pneumoniae infection and infectious mononucleosis (ie, EBV infection). Other viral infections, such as influenza, HIV, CMV, rubella, varicella, and mumps, have also been reported to be associated with a hemolytic anemia due to cold agglutinins. Associated illnesses also include subacute bacterial endocarditis, syphilis, and malaria. The development of a febrile illness in a patient with chronic cold agglutinin disease may also accelerate hemolysis.
CANOMAD syndrome
Cold agglutinins are seen in CANOMAD syndrome (chronic ataxic neuropathy ophthalmoplegia M-protein agglutination disialosyl antibodies). This syndrome is described by gait and upper-limb ataxia; cranial nerve involvement with external ophthalmoplegia; and the presence of cold agglutinins, IgM paraprotein, and anti-disialosyl antibodies. [7] The neurologic and hematologic symptoms have been seen to respond to rituximab. [8]
Malignancies
Lymphoproliferative and autoimmune diseases, myeloma, Kaposi sarcoma, and angioimmunoblastic lymphoma may occasionally be associated with the production of cold agglutinins. In a study of 78 patients with persistent cold agglutinins, 31 had lymphoma, 13 had Waldenström macroglobulinemia, 6 had chronic lymphoid leukemia, and 28 had chronic idiopathic cold agglutinin disease. [9]
A case of cold agglutinin–induced hemolytic anemia has been described in association with an aggressive natural killer cell (NK-cell) leukemia. [10] Nonhematologic malignancies can occasionally be associated with a high-titer cold agglutinin–induced hemolytic anemia. [11, 12]
Trisomy and translocation
Cytogenetic studies in patients with cold agglutinin disease have revealed the presence of trisomy 3 and trisomy 12. Translocation (8;22) has also been reported in association with cold agglutinin disease. [2, 13, 14]
Transplantation
Cold agglutinin–mediated hemolytic anemia has been described in living-donor liver transplant recipients taking tacrolimus and in bone marrow transplant recipients taking cyclosporine. It is postulated that such calcineurin inhibitors, which selectively affect T-cell function and spare B-lymphocytes, may interfere with the deletion of autoreactive T-cell clones, resulting in autoimmune disease. [15, 16, 17]
Systemic sclerosis
Cold agglutinin disease has been described in patients with sclerodermic features, with the degree of anemia correlating with increasing disease activity of the patient’s systemic sclerosis. This may suggest a close association between systemic rheumatic disease and autoimmune hematologic abnormalities. [18]
Hyperreactive malarial splenomegaly
Hyperreactive malarial splenomegaly (HMS) is an immunopathologic complication of recurrent malarial infection. Patients with HMS develop splenomegaly, acquired clinical immunity to malaria, high serum concentrations of anti-Plasmodium antibodies, and high titers of IgM, with a complement-fixing IgM that acts as a cold agglutinin. [19]
DPT vaccination
Diphtheria-pertussis-tetanus (DPT) vaccination has been implicated in the development of autoimmune hemolytic anemia caused by IgM autoantibody with a high thermal range. A total of 6 cases have been reported; 2 followed the initial vaccination and 4 followed the second or third vaccinations. [20, 21, 22, 23, 24]
Other
Equestrian perniosis (the development of tender, burning, nodular plaques on the thighs after horseback riding in cold weather) is a rare cause of persistent elevated titers of cold agglutinins. [25] Also rarely, the first manifestations of cold agglutinin disease can develop when a patient is subjected to hypothermia for cardiopulmonary bypass surgery. [26]
![]()
Pathophysiology
Cold agglutinins, or cold autoantibodies, occur naturally in nearly all individuals. These natural cold autoantibodies occur at low titers, less than 1:64 measured at 4°C, and have no activity at higher temperatures. Pathologic cold agglutinins occur at titers over 1:1000 and react at 28-31°C and sometimes at 37°C.
Cold agglutinin disease usually results from the production of a specific IgM antibody directed against the I/i antigens (precursors of the ABH and Lewis blood group substances) on red blood cells (RBCs). Cold agglutinins commonly have variable heavy-chain regions encoded by VH, with a distinct idiotype identified by the 9G4 rat murine monoclonal antibody. [27, 28, 29, 30, 9, 31, 32, 33, 34]
Because the I antigen is not activated until after birth, anti-i autoantibodies predominantly agglutinate neonatal RBCs, and anti-I autoantibodies predominantly agglutinate adult RBCs.
VH genes
The 9G4 idiotope is localized to the V4-34 encoded portion of the variable region. [35] It is found on cold agglutinin–producing malignant lymphoid cells in the bone marrow in persons with lymphoproliferative disorders and on a small proportion of normal lymphoid cells. In contrast, the cold agglutinins found in healthy individuals with no clinical symptoms are often derived from a variable segment other than the V4-34 portion. [36, 20]
The VH genes appear to regulate not only the production of cold agglutinins, but also the formation of normal antibodies to other carbohydrate antigens, both sharing the same fundamental mechanism of production. The I/i antigen analogs are present on human lymphocytes, neutrophils, and monocytes and in human saliva, milk, and amniotic fluid. Thus, in disease states, the finding of a clone of B-cells producing this antibody may be the result of the expansion of a normal clone that is specific for the production of an immunoglobulin with these properties. Autoimmune and lymphoproliferative disorders can also be associated with the production of cold agglutinins.
In vitro studies have shown that human monoclonal antibodies encoded by the V4-34 gene segment not only have cold agglutinin properties but also exhibit multireactivity. This is in contrast to the generally monospecific I/i reactivity of sera from patients with cold agglutinin disease. [33]
Associated infections
The hemolytic anemia associated with monoclonal cold agglutinins is typically more serious than that associated with polyclonal cold agglutinins. The monoclonal form is usually chronic, whereas the polyclonal form is often limited. [1]
Some polyclonal IgM cold agglutinins arise in association with infections with Mycoplasma pneumoniae, infectious mononucleosis, influenza B, and human immunodeficiency virus (HIV), as well as with other infections. Cold agglutinins develop in more than 60% of patients with infectious mononucleosis, but hemolytic anemia is rare. Hemolysis tends to develop 1-2 weeks after the onset of infectious mononucleosis, but it may occur simultaneously or up to 2 months after onset. [37] Cytomegalovirus (CMV), rubella virus, varicella-zoster virus (VZV), parvovirus B19, and Chlamydia psittaci have also been implicated. [37]
Increased expression of I/i antigens have been described on hemoglobin SS (HbSS) erythrocytes, which suggests that sickle cell disease may increase susceptibility to cold-mediated hemolysis. [38]
Antigen specificity
As with most autoimmune diseases of a chronic nature, cold agglutinin disease develops when stimulated B lymphocytes begin to produce pathogenic antibodies against an antigen that is normally present in human tissue. In cold agglutinin disease, the antibody is an IgM, usually monoclonal, with kappa (κ) or lambda (λ) light chains. In chronic cold agglutinin disease, the antibody is usually directed against the I antigen on the membrane of normal adult RBCs. Uncommonly, the antibody may be directed against only the i antigen found on fetal cord blood RBCs, which lack the mature I antigen; this has been reported in association with infectious mononucleosis. [39]
In a study of 78 patients, κ light-chain specificity was found in the majority of patients with chronic cold agglutinin disease or Waldenström macroglobulinemia, whereas two-thirds of cold agglutinins found in patients with lymphomas had λ light-chain specificity. The type of light chain appears to correlate with the antigen specificity of the cold agglutinin. Fifty-eight percent of IgM/κ (usually κIII variable region subgroup) was anti-I, but 75% of IgM/λ had other antigen specificities. [9]
Antigen specificities of cold agglutinins other than the I/i system that have been described include those against Pr, M, P, and Lud and anti-Gd, anti-Fl, and anti-Sa. [29, 30, 31] Exclusive occurrence of κ chains has also been shown with some cold agglutinins. [28] Thus, benign and malignant cold agglutinins exhibit differences in their light chains and their specificities toward membrane antigens.
Association of complement fixation with temperature
In vivo, the IgM antibody attaches to RBCs and causes them to agglutinate at temperatures below 37°C and maximally at 0-5°C, resulting in impaired blood flow to the digits, nose, and ears (ie, areas more likely to have colder temperatures [in the 30°C range]) when exposed to the cold.
Fixation of the C3 component of complement to the RBC by the cold agglutinin usually occurs in vivo at higher temperatures than those required by the IgM cold agglutinin to attach to the RBC, but it is generally less than 31°C. When the IgM/C3b-coated RBC circulates to warmer tissues, the IgM dissociates, leaving complement C3b on the original RBC.
The dissociated IgM cold agglutinin can then bind to another RBC at lower temperatures. Fixation of complement results in C3b and/or C4b components on the RBC membrane, which may lead to phagocytosis by macrophages in the reticuloendothelial system, particularly in the liver, where the macrophages have specific complement receptors. With time, the C3b components are converted enzymatically to C3dg, which is not recognized by macrophage receptors.
Complement levels in hemolysis
In chronic cold agglutinin disease, complement tends to be depleted. Thus, the hemolysis is self-controlled, and anemia may be only mild or moderate because these C3dg-coated RBCs are no longer capable of reacting with the IgM antibody in the cold, the C3dg-coated RBCs are not recognized by the macrophages, and low complement levels become rate-limiting.
Temporary increases in complement levels, as can occur with intercurrent febrile illnesses, can increase hemolysis. Lytic components of complement C5-C9 generally do not form on these cells, and intravascular hemolysis by complement is less likely to occur. [40] Hemolysis develops acutely following M pneumoniae infections and lasts approximately 1-3 weeks. Subclinical mild hemolysis with reticulocytosis may also occur, and the results of a direct Coombs test may be weakly positive, especially with M pneumoniae infections.
Underlying hematologic disease
A review of Mayo Clinic patients with cold agglutinin disease identified underlying hematologic diseases in 69 of 89 patients (76%). Monoclonal gammopathy of undetermined significance (MGUS) constituted 42 cases. The other hematologic disorders were lymphoproliferative disorders: macroglobulinemia, chronic lymphocytic lymphoma, other lymphomas (including low-grade B-cell and diffuse large B-cell lymphoma), and cutaneous T-cell lymphoma. [2]
Monoclonal cold agglutinin IgM antibodies found in patients with lymphoma are the product of the abnormal clone. Progression of an idiopathic cold agglutinin disease to malignant lymphoma may occur in some cases; thus, affected patients require close, long-term follow-up, given the obvious therapeutic implications. [39, 31] One study of 86 patients in Norway showed clonal light-chain predominance in 90% of patients, evidence of lymphoplasmacytic lymphoma in 50% of patients, and lymphoma of any type in 76% of patients overall. [2]
Warm-cold antibody combinations
Hemolysis due to cold agglutinins can sometimes be accompanied by a warm antibody (IgG), resulting in a mixed autoimmune hemolytic anemia. [39, 41] These patients have cold agglutinin syndrome and warm antibody autoimmune hemolysis, with the direct antiglobulin (direct Coombs) test results positive for the presence of IgG and complement on the surface of the sensitized RBC.
In mixed antibody syndromes, the IgG and IgM antibody components can be separated. The cold autoantibodies reactive at temperatures of 30°C or higher often show blood group specificity to the adult I antigen, whereas the warm autoantibodies are not directed against this system. A combination of cold agglutinins and cryoglobulins has also been reported with an IgM/κ monoclonal antibody, with specificity to the Pr2 antigen system. [34]
Biphasic hemolysins
The presence of biphasic hemolysins implicates more severe disease. Biphasic hemolysins bind to RBCs at low temperatures and activate complement to produce in vitro hemolysis at warmer temperatures (37°C), whereas monophasic hemolysins bind to RBCs and activate complement at the same temperature. [42]
Modulation of agglutinin production
Data have confirmed an immunomodulatory/immunosuppressive role of the naturally occurring anti-F(ab')2 antibodies in the production of cold agglutinins, with an inverse correlation between the titers of IgG-anti-F(ab')2 and cold agglutinins. [32] This inverse correlation was found only in patients with anti-I/i and in the presence of a monoclonal lymphocyte population.
Requirements for induction of active hemolytic anemia
Several factors play a role in determining the ability of a cold agglutinin to induce an active hemolytic anemia. [27, 2] These include the following:
-
Ability to initiate
-
Extent of antibody-induced complement activation
-
Concentration of the antibody
-
Range of temperatures, including the highest temperature at which the antibody interacts with the RBC (its thermal amplitude)
-
Qualitative binding of IgM to the RBC
-
Modification of the antibody's ability to fix complement components onto the RBCs
![]()
Epidemiology
Occurrence in the United States
The development of cold agglutinin syndrome is relatively uncommon, at least in the classic chronic form. Various reports state that 7-25% of cases of autoimmune hemolytic anemia (AIHA) are cold agglutinin mediated. A multi-database analysis found that the incidence of cold agglutinin disease ranged from 0.6 to 1.2 per 100,000 persons, while the 1-year prevalence ranged from 1.4 to 3.1 per 100,000 persons. [43]
International occurrence
Data regarding the incidence of cold agglutinin disease are lacking. Frequency figures listed for the United States probably also apply to Canada and the United Kingdom.
Berentsen et al calculated that the annual incidence of cold agglutinin disease in Norway is 1.9 cases per million population, while the prevalence is 20.5 cases per million population. In Lombardy, Italy, the annual incidence is 0.48 cases per million population and the prevalence is 5.0 cases per million population. The higher rates in Norway are likely due to the relatively colder outdoor temperatures there, compared with Italy, resulting in a higher proportion of patients experiencing symptomatic disease and being diagnosed. [44]
Sex- and age-related demographics
In general, no predilection for either sex is noted, although some report a female predilection in older populations. Autoimmune hemolytic anemia appears to be more common in male children and female adolescents. [45, 39]
Only rarely do Infants and children develop chronic cold agglutinin disease, although Mycoplasma pneumoniae and infectious mononucleosis are diseases of young persons. Chronic cold agglutinin disease typically affects adults who are of middle age and older, with an average age of older than 60 years and peaking in the seventh and eighth decades of life. Although found in persons of all age groups, mixed autoimmune hemolysis is also more frequent in later life.
![]()
Prognosis
Cold agglutinin disease may be associated with an excellent long-term prognosis if it is secondary to M pneumonia or viral infections that are, in themselves, self-limited. In children and young adults, acute hemolysis lasts 1-3 weeks; evidence of cold agglutinins disappears within 6 months.
Patients with the mildly to moderately severe primary (idiopathic) variety of cold agglutinin disease are expected to have a good long-term prognosis if excessive exposure to cold is avoided and with close medical surveillance for complications or progression to lymphoma.
The nature of the antigenic specificity of the cold agglutinin, as when it is directed against the Pr antigen system, may be associated with greater severity of disease.
Cold agglutinin disease associated with HIV infection may have a relatively poor prognosis due to the nature of the underlying disease. The same applies to cases associated with lymphoma, with the prognosis dependent on remission of the underlying malignancy.
Morbidity and mortality
Complications of cold agglutinin disease include the following:
-
Brisk hemolysis due to cold exposure
-
Ischemic complications at exposed sites due to prolonged cold exposure
-
Other symptoms related to severe anemia
-
Infrequently, development of malignant disease during follow-up care of a patient with idiopathic chronic cold agglutinin disease
-
Shock or congestive heart failure, resulting from severe hemolysis and anemia
-
Peripheral gangrene and, rarely, fatalities after inadvertent and perhaps prolonged exposure to the cold
Transfusions for life-threatening symptoms due to severe anemia require prewarming and the use of washed RBCs (not cold). In general, autoimmune hemolytic anemia has a mortality rate of 10%.
A study by Kamesaki et al indicated that the clinical characteristics of patients with autoimmune hemolytic anemia who have a positive direct Coombs test (direct antiglobulin test [DAT]) differ from those of patients with this type of anemia and a negative DAT. The report used data from 216 patients with autoimmune hemolytic anemia, including 154 who were DAT negative and 62 who were DAT positive. [46]
The investigators found that patients who were DAT negative tended to have milder anemia and hemolysis than did patients who were DAT positive and that they needed significantly lower steroid doses during maintenance treatment. The 2 groups of patients were found to have an equally good response to steroids. Survival at 1-year follow-up for each group was comparable to that of the other. [46]
![]()
Gertz MA. Updates on the Diagnosis and Management of Cold Autoimmune Hemolytic Anemia. Hematol Oncol Clin North Am. 2022 Apr. 36 (2):341-352. [QxMD MEDLINE Link].[Full Text].
Swiecicki PL, Hegerova LT, Gertz MA. Cold agglutinin disease. Blood. 2013 Aug 15. 122 (7):1114-21. [QxMD MEDLINE Link].[Full Text].
Małecka A, Trøen G, Tierens A, Østlie I, Małecki J, Randen U, et al. Immunoglobulin heavy and light chain gene features are correlated with primary cold agglutinin disease onset and activity. Haematologica. 2016 May 19. [QxMD MEDLINE Link].
Berentsen S, Randen U, Tjønnfjord GE. Cold agglutinin-mediated autoimmune hemolytic anemia. Hematol Oncol Clin North Am. 2015 Jun. 29 (3):455-71. [QxMD MEDLINE Link].
Maura F, Visco C, Falisi E, Reda G, Fabris S, Agnelli L, et al. B-cell receptor configuration and adverse cytogenetics are associated with autoimmune hemolytic anemia in chronic lymphocytic leukemia. Am J Hematol. 2012 Sep 26. [QxMD MEDLINE Link].
Khan FY, A yassin M. Mycoplasma pneumoniae associated with severe autoimmune hemolytic anemia: case report and literature review. Braz J Infect Dis. 2009 Feb. 13(1):77-9. [QxMD MEDLINE Link].
Delval A, Stojkovic T, Vermersch P. Relapsing sensorimotor neuropathy with ophthalmoplegia, antidisialosyl antibodies, and extramembranous glomerulonephritis. Muscle Nerve. 2006 Feb. 33(2):274-7. [QxMD MEDLINE Link].
Siddiqui K, Cahalane E, Keogan M, Hardiman O. Chronic ataxic neuropathy with cold agglutinins: atypical phenotype and response to anti-CD20 antibodies. Neurology. 2003 Nov 11. 61(9):1307-8. [QxMD MEDLINE Link].
Crisp D, Pruzanski W. B-cell neoplasms with homogeneous cold-reacting antibodies (cold agglutinins). Am J Med. 1982 Jun. 72(6):915-22. [QxMD MEDLINE Link].
Skorupa A, Chaudhary UB, Lazarchick J. Cold agglutinin induced autoimmune hemolytic anemia and NK-cell leukemia: a new association. Am J Hematol. 2007 Jul. 82(7):668-71. [QxMD MEDLINE Link].[Full Text].
Wortman J, Rosse W, Logue G. Cold agglutinin autoimmune hemolytic anemia in nonhematologic malignancies. Am J Hematol. 1979. 6(3):275-83. [QxMD MEDLINE Link].
Cao L, Kaiser P, Gustin D, Hoffman R, Feldman L. Cold agglutinin disease in a patient with uterine sarcoma. Am J Med Sci. 2000 Nov. 320(5):352-4. [QxMD MEDLINE Link].
Michaux L, Dierlamm J, Wlodarska L, et al. Trisomy 3q11-q29 is recurrently observed in B-cell non-Hodgkin's lymphomas associated with cold agglutinin syndrome. Ann Hematol. 1998 May. 76(5):201-4. [QxMD MEDLINE Link].
Chng WJ, Chen J, Lim S, et al. Translocation (8;22) in cold agglutinin disease associated with B-cell lymphoma. Cancer Genet Cytogenet. 2004 Jul 1. 152(1):66-9. [QxMD MEDLINE Link].
Kitamura T, Mizuta K, Kawarasaki H, Sugawara Y, Makuuchi M. Severe hemolytic anemia related to production of cold agglutinins following living donor liver transplantation: a case report. Transplant Proc. 2003 Feb. 35(1):399-400. [QxMD MEDLINE Link].
Tamura T, Kanamori H, Yamazaki E, et al. Cold agglutinin disease following allogeneic bone marrow transplantation. Bone Marrow Transplant. 1994 Mar. 13(3):321-3. [QxMD MEDLINE Link].
Thomson AW, Bonham CA, Zeevi A. Mode of action of tacrolimus (FK506): molecular and cellular mechanisms. Ther Drug Monit. 1995 Dec. 17(6):584-91. [QxMD MEDLINE Link].
Oshima M, Maeda H, Morimoto K, Doi M, Kuwabara M. Low-titer cold agglutinin disease with systemic sclerosis. Intern Med. 2004 Feb. 43(2):139-42. [QxMD MEDLINE Link].[Full Text].
Torres JR, Villegas L, Perez H, et al. Low-grade parasitaemias and cold agglutinins in patients with hyper-reactive malarious splenomegaly and acute haemolysis. Ann Trop Med Parasitol. 2003 Mar. 97(2):125-30. [QxMD MEDLINE Link].
Berentsen S, Beiske K, Tjonnfjord GE. Primary chronic cold agglutinin disease: an update on pathogenesis, clinical features and therapy. Hematology. 2007 Oct. 12(5):361-70. [QxMD MEDLINE Link].[Full Text].
Johnson ST, McFarland JG, Kelly KJ, Casper JT, Gottschall JL. Transfusion support with RBCs from an Mk homozygote in a case of autoimmune hemolytic anemia following diphtheria-pertussis-tetanus vaccination. Transfusion. 2002 May. 42(5):567-71. [QxMD MEDLINE Link].
Gunduz Gedikoglu A, Cantez T. Haemolytic-anaemia relapses after immunisation and pertussis. Lancet. 1967 Oct 21. 2(7521):894-5. [QxMD MEDLINE Link].
Zupanska B, Lawkowicz W, Gorska B, et al. Autoimmune haemolytic anaemia in children. Br J Haematol. 1976 Nov. 34(3):511-20. [QxMD MEDLINE Link].
Haneberg B, Matre R, Winsnes R, et al. Acute hemolytic anemia related to diphtheria-pertussis-tetanus vaccination. Acta Paediatr Scand. 1978 May. 67(3):345-50. [QxMD MEDLINE Link].
De Silva BD, McLaren K, Doherty VR. Equestrian perniosis associated with cold agglutinins: a novel finding. Clin Exp Dermatol. 2000 Jun. 25(4):285-8. [QxMD MEDLINE Link].
Agarwal SK, Ghosh PK, Gupta D. Cardiac surgery and cold-reactive proteins. Ann Thorac Surg. 1995 Oct. 60(4):1143-50. [QxMD MEDLINE Link].
Rosse WF, Adams JP. The variability of hemolysis in the cold agglutinin syndrome. Blood. 1980 Sep. 56(3):409-16. [QxMD MEDLINE Link].[Full Text].
Harboe M, van Furth R, Schubothe H, Lind K, Evans RS. Exclusive occurrence of K chains in isolated cold haemagglutinins. Scand J Haematol. 1965. 2(3):259-66. [QxMD MEDLINE Link].
Angevine CD, Andersen BR, Barnett EV. A cold agglutinin of the IgA class. J Immunol. 1966 Apr. 96(4):578-86. [QxMD MEDLINE Link].
Roelcke D. The Lud cold agglutinin: a further antibody recognizing N-acetylneuraminic acid-determined antigens not fully expressed at birth. Vox Sang. 1981 Nov-Dec. 41(5-6):316-8. [QxMD MEDLINE Link].
Roelcke D. Reaction of anti-Gd, anti-Fl and anti-Sa cold agglutinins with p erythrocytes. Vox Sang. 1984. 46(3):161-4. [QxMD MEDLINE Link].
Terness P, Kirschfink M, Navolan D, et al. Inverse correlation between IgG-antihinge region and antierythrocyte autoantibody in chronic benign and malignant cold agglutination. J Clin Immunol. 1997 May. 17(3):220-7. [QxMD MEDLINE Link].
Thorpe SJ, Turner CE, Stevenson FK, et al. Human monoclonal antibodies encoded by the V4-34 gene segment show cold agglutinin activity and variable multireactivity which correlates with the predicted charge of the heavy-chain variable region. Immunology. 1998 Jan. 93(1):129-36. [QxMD MEDLINE Link].[Full Text].
Ciejka JZ, Cook EB, Lawler D, et al. Severe cold agglutinin disease and cryoglobulinemia secondary to a monoclonal anti-Pr2 IgM lambda cryoagglutinin. Clin Exp Rheumatol. 1999 Mar-Apr. 17(2):227-31. [QxMD MEDLINE Link].
Potter KN. Molecular characterization of cold agglutinins. Transfus Sci. 2000 Feb-Apr. 22(1-2):113-9. [QxMD MEDLINE Link].
Jefferies LC, Carchidi CM, Silberstein LE. Naturally occurring anti-i/I cold agglutinins may be encoded by different VH3 genes as well as the VH4.21 gene segment. J Clin Invest. 1993 Dec. 92(6):2821-33. [QxMD MEDLINE Link].[Full Text].
McNicholl FP. Clinical syndromes associated with cold agglutinins. Transfus Sci. 2000 Feb-Apr. 22(1-2):125-33. [QxMD MEDLINE Link].
Maniatis A, Papayannopoulou T, Bertles JF. Fetal characteristics of erythrocytes in sickle cell anemia: an immunofluorescence study of individual cells. Blood. 1979 Jul. 54(1):159-68. [QxMD MEDLINE Link].[Full Text].
Sokol RJ, Booker DJ, Stamps R. Erythropoiesis: Paroxysmal Cold Haemoglobinuria: A Clinico-Pathological Study of Patients with a Positive Donath-Landsteiner Test. Hematology. 1999. 4 (2):137-164. [QxMD MEDLINE Link].
Packman CH, Leddy JP. Cryopathic hemolytic syndromes. Beutler E, Lichtman M, Coller B, Kippst, eds.Williams Hematology. 5th ed. New York, NY: McGraw-Hill; 1995. 685-91.
Sokol RJ, Hewitt S, Stamps BK. Autoimmune hemolysis: mixed warm and cold antibody type. Acta Haematol. 1983. 69(4):266-74. [QxMD MEDLINE Link].
Sokol RJ, Booker DJ, Stamps R, Walewska R. Cold haemagglutinin disease: clinical significance of serum haemolysins. Clin Lab Haematol. 2000 Dec. 22(6):337-44. [QxMD MEDLINE Link].
Bozzi S, Umarje S, Hawaldar K, Tyma J, Ward B, Schinkel J, et al. Prevalence and incidence of primary autoimmune hemolytic anemia and cold agglutinin disease in the United States, 2016-2023. PLoS One. 2025. 20 (6):e0323843. [QxMD MEDLINE Link].[Full Text].
Berentsen S, Barcellini W, D'Sa S, et al. Cold agglutinin disease revisited: a multinational, observational study of 232 patients. Blood. 2020 Jul 23. 136 (4):480-488. [QxMD MEDLINE Link].[Full Text].
Dacie J, The auto-immune haemolytic anaemias. The Haemolytic Anaemias. 3rd ed. Edinburgh, United Kingdom: Churchill Livingstone; 1992. Vol 3.: 210-362.
Kamesaki T, Toyotsuji T, Kajii E. Characterization of direct antiglobulin test-negative autoimmune hemolytic anemia: A study of 154 cases. Am J Hematol. 2012 Oct 25. [QxMD MEDLINE Link].
Berentsen S. How I treat cold agglutinin disease. Blood. 2021 Mar 11. 137 (10):1295-1303. [QxMD MEDLINE Link].[Full Text].
Berentsen S. New Insights in the Pathogenesis and Therapy of Cold Agglutinin-Mediated Autoimmune Hemolytic Anemia. Front Immunol. 2020. 11:590. [QxMD MEDLINE Link].[Full Text].
Garratty G, Petz LD, Hoops JK. The correlation of cold agglutinin titrations in saline and albumin with haemolytic anaemia. Br J Haematol. 1977 Apr. 35(4):587-95. [QxMD MEDLINE Link].
Piatek C, Murakhovskaya I, Karaouni A, Miles G, Bozzi S, Heller C, et al. Real-World Use of Rituximab in the Treatment of Cold Agglutinin Disease in the United States: A Retrospective Study. EJHaem. 2025 Aug. 6 (4):e70082. [QxMD MEDLINE Link].
Berentsen S, Randen U, Vagan AM, Hjorth-Hansen H, Vik A, Dalgaard J. High response rate and durable remissions following fludarabine and rituximab combination therapy for chronic cold agglutinin disease. Blood. 2010 Oct 28. 116(17):3180-4. [QxMD MEDLINE Link].
Röth A, Bommer M, Hüttmann A, Herich-Terhürne D, Kuklik N, Rekowski J, et al. Eculizumab in cold agglutinin disease (DECADE): an open-label, prospective, bicentric, nonrandomized phase 2 trial. Blood Adv. 2018 Oct 9. 2 (19):2543-2549. [QxMD MEDLINE Link].[Full Text].
Roman E, Fattizzo B, Shum M, Hanna W, Lentz SR, Araujo SSS, et al. Safety and efficacy of pegcetacoplan treatment for cold agglutinin disease and warm antibody autoimmune hemolytic anemia. Blood. 2025 Jan 23. 145 (4):397-408. [QxMD MEDLINE Link].[Full Text].
Mohamed A, Alkhatib M, Alshurafa A, El Omri H. Refractory cold agglutinin disease successfully treated with daratumumab. A case report and review of literature. Hematology. 2023 Dec. 28 (1):2252651. [QxMD MEDLINE Link].
Jalink JM, Jacobs CFJ Dr, Khwaja JK, Evers DE, Bruggeman CB, Fattizzo BF, et al. Daratumumab monotherapy in refractory warm autoimmune hemolytic anemia and cold agglutinin disease. Blood Adv. 2024 Mar 20. [QxMD MEDLINE Link].
Fattizzo B, Pedone GL, Brambilla C, Pettine L, Zaninoni A, Passamonti F, et al. Recombinant erythropoietin in autoimmune hemolytic anemia with inadequate bone marrow response: a prospective analysis. Blood Adv. 2024 Mar 12. 8 (5):1322-1327. [QxMD MEDLINE Link].[Full Text].
Moser MM, Jilma B. Add-on erythropoietin in autoimmune hemolytic anemia. Blood Adv. 2024 Mar 12. 8 (5):1320-1321. [QxMD MEDLINE Link].[Full Text].
Hoppe B, Gaedicke G, Kiesewetter H, Salama AR. Response to intravenous immunoglobulin G in an infant with immunoglobulin A-associated autoimmune haemolytic anaemia. Vox Sang. 2004 Feb. 86(2):151-3. [QxMD MEDLINE Link].
Roy-Burman A, Glader BE. Resolution of severe Donath-Landsteiner autoimmune hemolytic anemia temporally associated with institution of plasmapheresis. Crit Care Med. 2002 Apr. 30(4):931-4. [QxMD MEDLINE Link].
Teachey DT, Felix CA. Development of cold agglutinin autoimmune hemolytic anemia during treatment for pediatric acute lymphoblastic leukemia. J Pediatr Hematol Oncol. 2005 Jul. 27(7):397-9. [QxMD MEDLINE Link].
Giulino LB, Bussel JB, Neufeld EJ. Treatment with rituximab in benign and malignant hematologic disorders in children. J Pediatr. 2007 Apr. 150(4):338-44, 344.e1. [QxMD MEDLINE Link].[Full Text].
Berentsen S, Ulvestad E, Tjonnfjord GE. B-lymphocytes as targets for therapy in chronic cold agglutinin disease. Cardiovasc Hematol Disord Drug Targets. 2007 Sep. 7(3):219-27. [QxMD MEDLINE Link].
Berentsen S, Randen U, Oksman M, Birgens H, Tvedt THA, Dalgaard J, et al. Bendamustine plus rituximab for chronic cold agglutinin disease: results of a Nordic prospective multicenter trial. Blood. 2017 Jul 27. 130 (4):537-541. [QxMD MEDLINE Link].
Jäger U, Barcellini W, Broome CM, Gertz MA, Hill A, Hill QA, et al. Diagnosis and treatment of autoimmune hemolytic anemia in adults: Recommendations from the First International Consensus Meeting. Blood Rev. 2020 May. 41:100648. [QxMD MEDLINE Link].
Sandip Panicker, Graham C. Parry, Michael Fillitz, et al. TNT009, a monoclonal antibody inhibitor of C1s, induces a rapid and complete remission of anemia in primary cold agglutinin disease patients. Immunobiology. 2016 Oct 01. 221:1170-1171.
Röth A, Barcellini W, D'Sa S, et al. Inhibition of Complement C1s with Sutimlimab in Patients with Cold Agglutinin Disease (CAD): Results from the Phase 3 Cardinal Study. Blood. 2019. 134 (Supplement_2):LBA-2. [Full Text].
Röth A, Barcellini W, D'Sa S, Miyakawa Y, Broome CM, Michel M, et al. Sutimlimab in Cold Agglutinin Disease. N Engl J Med. 2021 Apr 8. 384 (14):1323-1334. [QxMD MEDLINE Link].[Full Text].
Röth A, Berentsen S, Barcellini W, D'Sa S, Jilma B, Michel M, et al. Sutimlimab in patients with cold agglutinin disease: results of the randomized placebo-controlled phase 3 CADENZA trial. Blood. 2022 Sep 1. 140 (9):980-991. [QxMD MEDLINE Link].[Full Text].
Gelbenegger G, Schoergenhofer C, Derhaschnig U, Buchtele N, Sillaber C, Fillitz M, et al. Inhibition of complement C1s in patients with cold agglutinin disease: lessons learned from a named patient program. Blood Adv. 2020 Mar 24. 4 (6):997-1005. [QxMD MEDLINE Link].[Full Text].
Kobayashi H, Ouchi T, Kitamura W, Asakura S, Yano T, Takeda H, et al. Sutimlimab suppresses SARS-CoV-2 mRNA vaccine-induced hemolytic crisis in a patient with cold agglutinin disease. J Clin Exp Hematop. 2023. 63 (4):246-250. [QxMD MEDLINE Link].[Full Text].
Fattizzo B, Röth A, Broome CM, Khan U, Wardęcki M, Cordoba M, et al. COVID-19 vaccine safety and immunogenicity in patients with cold agglutinin disease receiving concomitant sutimlimab. Am J Hematol. 2024 Apr. 99 (4):789-791. [QxMD MEDLINE Link].
Shapiro R, Chin-Yee I, Lam S. Eculizumab as a bridge to immunosuppressive therapy in severe cold agglutinin disease of anti-Pr specificity. Clin Case Rep. 2015 Nov. 3 (11):942-4. [QxMD MEDLINE Link].
Inaba H, Geiger TL, Lasater OE, Wang WC. A case of hemoglobin SC disease with cold agglutinin-induced hemolysis. Am J Hematol. 2005 Jan. 78(1):37-40. [QxMD MEDLINE Link].[Full Text].
Batalias L, Trakakis E, Loghis C, et al. Autoimmune hemolytic anemia caused by cold agglutinins in a young pregnant woman. J Matern Fetal Neonatal Med. 2006 Apr. 19(4):251-3. [QxMD MEDLINE Link].
Atkinson VP, Soeding P, Horne G, Tatoulis J. Cold agglutinins in cardiac surgery: management of myocardial protection and cardiopulmonary bypass. Ann Thorac Surg. 2008 Jan. 85(1):310-1. [QxMD MEDLINE Link].
Aoki A, Kay GL, Zubiate P, Ruggio J, Kay JH. Cardiac operation without hypothermia for the patient with cold agglutinin. Chest. 1993 Nov. 104(5):1627-9. [QxMD MEDLINE Link].
Barbara DW, Mauermann WJ, Neal JR, Abel MD, Schaff HV, Winters JL. Cold agglutinins in patients undergoing cardiac surgery requiring cardiopulmonary bypass. J Thorac Cardiovasc Surg. 2013 Sep. 146(3):668-80. [QxMD MEDLINE Link].
Hippe E, Jensen KB, Olesen H, Lind K, Thomsen PE. Chlorambucil treatment of patients with cold agglutinin syndrome. Blood. 1970 Jan. 35(1):68-72. [QxMD MEDLINE Link].[Full Text].
-
Peripheral blood smear showing several clumps of RBCs with the largest in the center. These are typical of aggregates seen in persons with cold agglutinin disease.
-
Blood smear showing spherocytic and agglutinated red blood cells.
