Do viruses trigger Alzheimer's?
economist.comVery interesting.
Memantine is an antiviral/nootropic (NMDA agonist) that's considered one of the best conventional therapies for Alzheimer's. For e.g., https://pubmed.ncbi.nlm.nih.gov/32914577/
Amantadine is a related compound that's seemingly more potent as an antiviral, and less potent at the NMDA receptor.
Medical hypothesis: This makes me wonder if amantadine might be an effective drug in Alzheimer's treatment. It would come as a total shock to the med chem community if memantine's activity had to do with its suppression of viral replication, and much less to do with its activity at the NMDA receptor.
As an aside, the Russians have a similar drug called bromantane which is sold OTC as a sort of mental energy booster. It's not really a stimulant, and its effects are mild enough for daily use. It might also be very interesting in this context. https://en.wikipedia.org/wiki/Bromantane
I've had some experience here and will add a couple notes.
Memantine has been useful for slowing down Alzheimer's and temporarily improving responsiveness. However, Memantine has not shown any effectiveness in reversing Alzheimer's or fully stopping its progression (sadly). Memantine does seem to increase self-awareness clarity but, counterintuitively, seems to also disrupt memory recall. Word of caution, in one rat study, I had read that Memantine could have long term side-effects of hindering memory recall.
Amantadine has a fascinating structure, but it seems like it's not super useful by itself from studies. It seems more like a very promising 'base structure' to build future compounds upon (like Memantine and bromantane).
Anyways, this family is rather interesting for a number of its properties and are still not very well known or understood. Please do share any more insights.
Random notes:
- Unlike amantadine, chemically-related tromantadine is potently effective against HSV. https://pmc.ncbi.nlm.nih.gov/articles/PMC185716/
- There's another paper which may shed some light on the herpes-Alzheimer's connection, and it notes that treatment with tromantadine (among others) is starkly beneficial: https://pmc.ncbi.nlm.nih.gov/articles/PMC5935641/
- If the connection is established, it could be that a tromantadine-like molecule with activity against herpes simplex -- plus mild activity at the NMDA receptor reducing excitotoxicity and protecting neurons -- could potentially be a good prophylactic against Alzheimer's.
- It would be interesting to test amide-linked amantadine-phenylalanine and memantine-phenylalanine conjugates. Such things would probably penetrate the BBB very well, as they could take advantage of amino acid transporters. (The LAT1 transporter in particular.) And they resemble tromantadine -- where it is said that the amide itself is a necessary moiety in countering HSV. Structure: https://i.ibb.co/7tS4MGGL/Amantadine-Phe.png
Are you a drug developer by trade? You certainly think like someone who’s seen some SARs…
Thanks, man. I'm more of a general-purpose chemist. I've done medicinal chemistry for drug development, but also inorganic compound development, metallurgy, all kinds of other stuff. It's a broad and fun field.
Very cool. I’m a bloodhound for spotting talent. Are you still in the space?
Yeah, and in fact working on some interesting projects. Feel free to email me if you'd like to chat: jakeganor [at] gmail
Super cool :) Do you have a preferred social media handle to follow for any future adamantane and other related research posts?
Afraid not. I only post here, lol
I believe most nootropics work for Alzheimer's, probably Huperzine A, too. Perhaps even Noopept.
NMDA agonists and acetylcholinesterase (they inhibit the breakdown of the neurotransmitter acetylcholine) in general.
Benadryl (DPH) and first-generation antihistamines are the opposite of that, they can cause delirium (and it messes up your memory and cognition in general) and whatnot, they are anticholinergic, some more than others. I had anticholinergic toxicity from DPH before.
I take Alpha-GPC (a very soluble form of choline) and Huperzine A for cognition / memory, others couple it with racetams (e.g. piracetam, pramiracetam, aniracetam, etc.).
My primary care doctor is telling all of her patients not to take Zyrtec for an anti-histamine because it is causing dementia side effects in her older patients. Antecdotal but interesting.
For the reasons I mentioned, yes. :)
But Zyrtec is second-generation. It shows 20,000-fold or greater selectivity for the H1 receptor over the five muscarinic acetylcholine receptors, and hence does not exhibit anticholinergic effects, so it should be OK. May still cause drowsiness, however.
What about desloratadine?
Desloratadine (Clarinex, Aerius) is a selective H1-antihistamine which functions as an inverse agonist at the histamine H1 receptor.
From Wikipedia:
> At very high doses, it is also an antagonist at various subtypes of the muscarinic acetylcholine receptors. This effect is not relevant for the drug's action at therapeutic doses.
Thus, it is an anticholinergic only at very high doses, and it does not readily pass the BBB, therefore drowsiness is NOT likely (probably at very high doses only). At any rate, it does not affect the CNS at therapeutic doses, so memory / cognition issues, along with drowsiness are not an issue.
FWIW "2% of Caucasians and 18% of people from African descent are desloratadine poor metabolizers.", meaning "In these people, the drug reaches threefold higher plasma concentrations at seven hours after intake, and it has a half-life of 89 hours (compared to a 27-hour half-life in normal metabolizers). Adverse effects were reported at similar rates in poor metabolizers, suggesting that it is not clinically relevant.".
Is BBB == "blood-brain barrier"?
Yes.
Do you know if there are any SNPs correlated with poor desloratadine metabolizers?
I do not think that there are any definitive single nucleotide polymorphisms (SNPs) currently known to be specifically correlated with poor desloratadine metabolism.
I think perhaps the genetic variation in the enzymes involves in its metabolism like UGT2B10 and CYP2C8 may contribute to differences in metabolism. There is just no conclusive identification of specific SNPs that definitively determine poor metabolizer status. The precise genetic variants (if any) have not yet been definitively pinpointed.
For all we know, the differences may be attributable to variations in study design, sample sizes, definition of what constitutes a "poor metabolizer", and genetic heterogeneity among populations. Some reported rates of poor metabolizers vary, some studies report around 7% overall and 20% in African descent individuals, while others suggest the figures I have mentioned. There was a somewhat recent randomized study in healthy Chinese subjects, and found no statistically significant association between the UGT2B10 or CYP2C8 genotypes.
What is clear is that while genetic factors are likely involved and poor metabolizer phenotype exists for the drug, no single genetic marker has yet been found to predict poor metabolism of this drug, and there is a notable interethnic difference in desloratadine metabolism.
TL;DR: Currently there is no definitive evidence linking specific SNPs to poor desloratadine metabolism, but genetic variation in enzymes like UGT2B10 and CYP2C8 is implicated, but further research is needed.
I hope this answers your question, but the bottom line is that more research is needed. If you know something, let me know though!
Interesting, and thank you for the informative response. I have very weird reactions to cholinergic/anticholinergic drugs ranging from severe hallucinations to massive impacts to working memory. I've always figured there is something unique about that part of my biology but don't really no where to look to try and identify why.
I have weird or controversial reactions to most medications, especially psychiatric and drugs. I have no clue why. I have MS, I have brain lesions, they might play a part.
- For example nothing happened from 190 x 1 mg alprazolam + 0.5 L whiskey.
- None of the psychiatric medications worked for me (tried almost all there is, it took a long time). No pros, nor cons.
- Opiates do not cause euphoria, nor sedation for me. Without tolerance.
- The list goes on...
I have never figured out why medications affect me extremely differently from other people.
I took 5 x 50 mg DPH, nothing happened, then the next day I took it again, and I got anticholinergic toxicity. Perhaps it accumulated in this case, but yeah, it was one of the worst experiences I have had (delirium with dysphoric hallucinations, cognitive decline, memory issues). Took me months to recover. I have had auditory hallucinations for a couple of days, too.
What cholinergics and anticholinergics have you tried and what were your experiences?
I advise against taking aGPC because it is very much associated with TMAO production due to adverse gut fermentation, leading to harmful effects on blood vessels. Switch to citicoline which doesn't look to have this issue.
Yes, Citicoline is great, too, I agree. As long as it is not Choline bitartrate (most common form) which is pretty useless, the body cannot utilize it whatsoever.
As for what you said regarding alpha-GPC, it is somewhat true:
> Although alpha-GPC is largely considered to be safe due to its structural feature, multiple studies have indicated that a high plasma choline level is associated with an increased risk of cardiovascular disease through trimethylamine-N-oxide (TMAO) produced by gut microbiota from choline. Some studies have highlighted that TMAO increases the likelihood of stroke and cardiovascular disease.11
> In line with this observation, a recent animal model study revealed that even though alpha-GPC supplements improved neurological functions, they increased the risk of atherosclerosis in hyperlipidemic rats. In the future, scientists must elucidate the possible mechanism that associates alpha-GPC with increased cardiovascular risks.
https://examine.com/supplements/alpha-gpc/?show_conditions=t...
https://www.news-medical.net/health/Alpha-GPC-What-Science-S...
https://pmc.ncbi.nlm.nih.gov/articles/PMC8708068/
https://www.sciencedirect.com/science/article/pii/S002192582...
That said, "However, the currently available evidence is preliminary in nature, so randomized controlled trials and large cohort studies are needed to confirm these findings.".
Oh also, it says "multiple studies have indicated that a high plasma choline level is associated with an increased risk of cardiovascular disease", but I wonder why it does not apply to CDP-Choline (Citicoline) since it does increase plasma choline level, too, but perhaps not as highly? I am not sure of the exact mechanisms.
BTW Citicoline's other name is CDP-Choline, forgot to edit in time.
My doc put my on amantadine for post covid symptoms and I felt like it gave me mild dementia and had to stop :/
edit: Fun fact, the side effects were so bad I made a very big mishap that destroyed a (very very expensive) f-class flight simulator.
Memantine is an NMDA antagonist like ketamine and other dissociatives.
Memantine is in no way a disassociative though at therapeutic doses. It also has dopaminergic activity which manifests gradually over months while the NMDAr antagonist activity dials down.
{kind=link}
I think there is something to viruses being a big agent of aging. I'm 40 and recently came down with a bad case of norovirus, followed by some kind of flu-like thing. 3 weeks of illness. Afterwards, I felt as if I had aged 10 years, and looking into the mirror it was like looking at what I will probably look like at 50.
It made me wonder how much of aging is mediated by damage from infection, which we fight off, but come out of weaker for it.
It certainly makes me want to double check all my vaccines, and once my kids are older, practice a little better hygiene including things like masking up in tight spaces (pretty much impossible with a 6 and 9 year old in the house, they are the vector right now).
One that i recently experienced is 'reactive athritis' which is a form of athritis commonly experienced after a stomach virus.
If you start looking into it it's due to an immune response that occurs in people with the https://en.wikipedia.org/wiki/HLA-B27 gene and that gene is associated with a large number of athritis risk factors (but also resistance to a lot of things including HIV).
I've had the same. It took over 5 years for me to go back to normal. Apparently somewhat common, but rarely talked about. And any virus can cause it.
Reactive arthritis is easy to treat using a course of appropriate antibiotics, although the right choice may vary. A good powerful blend of probiotics in a capsule also helps tremendously although it's not sufficient without the antibiotic. I have used this approach to treat it. For an acute case, also consider activated carbon. Obviously the three all oppose each other, so take them at separate times.
As for pathogenic viruses in the gut, immune boosting supplements, glutamine, and collagen should help with treatment.
Getting sick is a very stressful period, physically and mentally. It absolutely ages you.
We're sick far less often nowadays. Common illnesses were more common in previous generations. Back in the day "everyone got measles".
While people fear being "too clean" there is also a downside to being "too exposed".
https://en.wikipedia.org/wiki/Hygiene_hypothesis
The hygiene hypothesis does not suggest that having more infections during childhood would be an overall benefit
Important to take certain antioxidants and supplements after. Plus whole good food. Focusing heavily on good sleep and rest (so hard). And doing some level of exercise, but even just starting with walking.
I had a post viral effect after Covid. But maybe 2 months. Then I finally took it easy with working out and it went away.
> A group of researchers mostly based at Columbia University are testing whether valacyclovir, an antiviral used against HSV1, can slow down cognitive decline in people with early stage Alzheimer’s. Between 2018 and 2024, the researchers recruited 120 patients and treated half with the antiviral.
Outsider view: while I'm excited we're making progress, I can't shake a feeling of sadness that the best we could manage was a study this small, started 7 years ago. If it's as pivotal as the article suggests, one would hope we could get more than 60 people in the experimental arm (IIUC this antiviral is widely prescribed, well-tolerated, and off-patent). Nonetheless, excited to see the outcome
> off-patent
Well there’s your problem: no one can make money off of it, unless they develop a new delivery mechanism, etc.
Patents encourage developing new medicines, but not developing new knowledge about (never mind use of) old medicine.
The solution (in the US) is obvious: federal funding of research that stands to help lots of people but not make lots of money. Since most of these patients (in the US) are going to be on Medicare, there could be huge potential cost savings to the taxpayer: memory care is EXPENSIVE, so even the paltry amount covered by Medicare racks up (and the opportunity costs of people paying for private memory care is enormous).
But instead of increasing funding for this kind of life- AND MONEY-saving research, this administration is freezing and slashing research funding, and specifically targeting Columbia for political/Trump’s-petty-grudge reasons.
> Well there’s your problem: no one can make money off of it
You can patent new applications of an existing drug. This has been somewhat of a problem, as companies can just look at how drugs are being used off-label, and patent some of these uses.
People are doing this with vetinary drugs too. A company called Tarsus Pharmaceuticals recently developed a drug called xdemvy by repurposing an anti-flea drug for dogs. It basically cures an eyelid condition called demodex blepharitis. They're a $2b company now.
They barely had to do any new science. It just took some creativity and almost $250m worth of clinical trials.
I suspect the lucrative patent system has helped create rather exorbitant costs and restrictions for performing trials, which hinders non-patentable research, ironically.
But both the federal and state govts do fund tons of such research. Some states have specific Alzheimer's trials and funds. I would think they could handle dirt-cheap therapies like this without getting into sweeping political changes. Though I suspect the solution is much harder than just run a trial with the drugs we have, or else we would already be hearing about mountains of evidence from doctors using the medications off-label.
>Well there’s your problem: no one can make money off of it, unless they develop a new delivery mechanism, etc.
You hit the nail on the head. Ketamine is a generic drug that costs next to nothing; Spravoto (ketamine-derived nasal spray) is already a billion dollar/year drug for Johnson & Johnson, with prospects of $5 billion/year.
Source: https://archive.ph/rzqxt [Wall Street Journal]
Worth mentioning that the evidence says that patents don't have an effect on new drug creation/inventions. Evidence is collected here http://www.dklevine.com/general/intellectual/againstfinal.ht..., pretty neat to know that Italy/Switzerland had a patentless pharma industry until quite recently.
Having said that, I think you're right that under this system, research/capital definitely gets directed in a different way.
A major reason Alzheimer's research hasn't advanced in the last 25 years is that patents aren't long enough to study it. Remember: patents don't kick in after the FDA approved your drug. It's after you develop it. That's why ozempic is going off-patent in a just few years even though it's a new product. They patented it a long time ago.
With Alzheimer's though, the clinical trials are going to take a long time. Probably 10 years at least, because our current understanding of the disease is that it begins in your mid to late 40s, and only manifests as severe memory loss decades later. Our current method of trying to treat it is like putting someone in pallatiave care with stage 12 cancer through chemo. Just doesn't work.
But drug companies have no choice because if they run 10-15 year trials, their drug will be off patent before the FDA/EMA even looks at it.
If I were King for a day, one thing I'd do is a blanket 40 year patent life on Alzheimer's drugs. It's worth the cost. This disease will bankrupt every nation otherwise.
While I understand the narrative you're proposing, what I brought with my source was a collection of evidence where pharmacological innovation happened at an unaltered rate pre and post patents in e.g. Italy and Switzerland. While I understand the hypothesis of "Pharma innovation, due to high costs of entry, only happens (or is greatly improved) when guaranteed a monopoly", it doesn't seem to be backed by the data.
I agree with you in principle though - if all that were stopping us from achieving a cure were a 40 year patent, I would support your 1-day monarchy in a heartbeat.
Chapters 9 and 10 of the book cover this in more detail if you're interested (very self-contained).
This is bullshit. Drug research costs money, A LOT OF MONEY. A new drug right now costs somewhere around $5 billion, mostly because 90% of drugs fail in trials.
mRNA vaccines, semaglutide, mAB therapies, none of these would have happened without patents as an incentive.
Then why is it that when pharma patents were introduced in countries that didn't have them, the rate of innovation, TFP, R&D-as-%-GDP didn't increase? I brought a source to this debate, if you have sources showing that increases in patent scope, length, or introduction of patents increased pharamacological innovation I'd love to see it - I'm going down this rabbit hole now and am collecting info.
Another interesting one is [1] where they asked readers of the BMJ to vote on the top 15 most important medical milestones. Of the 15, only the contraceptive pill and Chlorpromazine had anything to do with patents.
In [2] the "Chemical and Engineering News magazine" collected a list of top pharmaceuticals (46 total). To quote the book I linked:
> Patents had pretty much nothing to do with the development of 20 among the 46 top selling drugs [..] . For the remaining 26 products patents did play an important role [..]. Notice though that of these 26, 4 were discovered completely by chance and then patented (cisplatin, librium, taxol, thorazin), 2 were discovered in university labs before the Bayh-Dole Act was even conceived (cisplatin and taxol). Further, a few were simultaneously discovered by more than one company leading to long and expensive legal battles, however, the details are not relevant to our argument.
Regarding the cost of drug trials, they cover this well in Chapters 9 and 10, I found it quite interesting.
Regarding how else companies make money without being granted temporary govt-backed monopolies, Chapter 6 covers both the theoretical and real-life examples.
[1] https://www.bmj.com/content/medical-milestones [2] https://pubsapp.acs.org/cen/coverstory/83/8325/8325list.html
Quite an interesting attempt to advance the general process is DeepMind's project to make a cell simulation so you can try chucking in drugs into the simulation and see what they would do quicker than in the lab/patients. They are talking about having a simple cell up in five years. Hassabis talking about it: https://youtu.be/CEOOMYxMvY4
This article is all the supporting evidence without any of the setbacks and failures at reproducing the correlations. There have been attempts at showing benefits with antivirals before. Just not a full-on double-blind study apparently. I recall reading about a study with high doses that showed no benefit for people in early stages.
The 7 years time duration probably comes from the size of the study and also how long it is believed to take to get benefit if there is one. I would think if it really worked they would have stopped early for ethics reasons because they should also give the treatment to the placebo arm rather than watch them decline while knowing how to prevent it.
>If it's as pivotal as the article suggests
Let's be honest, this is a longshot.
90% of drug trials fail. Shows you how primitive our accepted practice is. Where else is a 90% failure considered to be an acceptable outcome?
Ycombinator startups?
We cannot ignore that we know so little about how Alzheimer's works, we are potentially lumping multiple diseases under the same label.
The amyloid hypothesis doesn't have to be wrong for the T3D to be true, and the viral potential to also be true if we are looking at 3-5 different diseases that have similar presentations. This also somewhat suggests why it may be the most common form of dementia.
I work in the neurotech/sleeptech space (https://affectablesleep.com) and there is a strong link between sleep quality and Alzheimer's. It is theorized that AD is more common in women due to the lack of sleep through child-rearing and menopause, which decreases the brain's ability to remove amyliod/tau. Of course, this is only relevant to the amyliod hypothesis.
I don't know what it looks like from the perspective of someone in the field, but just as someone who is interested in this sort of stuff, it seems more and more plausible that quite many of diseases that have grown more prevalent in the last century, especially autoimmune diseases, are cause by viruses.
It makes sense: the viral pressure has increase by a lot due to both increase in population density and increased travel across the world. At the same time there has been an increase in many autoimmune diseases, many types of cancer, Alzheimer's disease, etc. Also, from some proven cases, we know that viruses can trigger serious diseases (MS disease, type 1 diabetes).
I have both T1D and MS. For MS, one leading idea is that getting exposed to Mono later in life can trigger the disease. There’s solid evidence for this.
For T1D, it’s similar - there’s a notion that you’re genetically predisposed to it and certain types of infections during adolescence can cause it to manifest.
I’ve had discussions with researchers in the space and apparently certain autoimmune diseases happen less often in “grubbier” parts of the world (their words, not mine) even when the population density is high, and an inference here is that >early exposure< to certain infections might not trigger some of these problematic autoimmune reactions.
Side note: these diseases aren’t fun, especially when working in tech. I’m appreciative of those dedicating their lives to researching autoimmune disease.
> I’ve had discussions with researchers in the space and apparently certain autoimmune diseases happen less often in “grubbier” parts of the world
Is that corrected for mortality? It seems like an analysis like that would be quite prone to survivor bias.
For MS in particular there's several EBV mRNA vaccines in clinical trials - not just to prevent mono itself, but also to prevent long term complications (theoretically including MS) for people who already had it.
Has viral pressure really increased? It seems stuff spread globally a few generations ago with things like the flu in the early 1900s. Even in the middle ages you had stuff like the plague.
What has changed is the sterility of our environment. Better bathing, more hand washing, food safety rules, etc. There have been theories that autoimmune diseases might be increasing because we aren't exposed to enough "normal" pathogens.
I'm highly suspicious that higher viral pressures are the cause of increasing dementia rates, as it seems we're exposed to less today.
Bacterial, fungal and parasitic load has lessened, for sure, due to sterility of the environment, because many of those come from exposure to animals and plants. But viral load from viruses that spread from human-to-human and live exclusively in humans has increased because there are more humans and they spread the diseases around the world more effectively than before.
Yes, we probably get way less pathogens overall than we used to, but at the same time we get more pathogens that live exclusively on humans (such as respiratory viruses).
> But viral load from viruses that spread from human-to-human and live exclusively in humans has increased because there are more humans and they spread the diseases around the world more effectively than before.
This seems like pure conjecture to me, and without any actual evidence to support it, I'm disinclined to believe it. My guess is that the number of people any one individual interacts with has gone down considerably since the beginning of the century, and earlier. Before the advent of the car, shared forms of travel were much more common. People do much less forms of basic shopping than they used to given the rise of the Internet. Air travel, while much faster, is much less crowded that the ship travel of earlier generations.
> Before the advent of the car, shared forms of travel were much more common. Air travel, while much faster, is much less crowded that the ship travel of earlier generations.
Maybe in the US. Definitely not in most of the world. For my grandparent 70 years or so ago, the way to travel long distances was riding a donkey. Now travel by bus, train, subway, etc. is really common and something that most people experience often. 100 years ago of course there were trains, stagecoaches, boats, etc. but they were for a tiny minority of society or for special occasions (like to migrate a different continent to not return in decades, etc.). I'm also pretty sure air travel has a much higher penetration than ship travel would have 100 years ago.
As further anec-data points, there are much more massive gatherings now (concerts, sports, etc. - church used to be the major gathering, but churches tend to be ample and ventilated). And every parent knows that daycare and kindergarten are a major vector for pathogens. I used to get like a cold a year with 2 days mild congestion, and since my kid started kindergarten (he didn't go to daycare) we all started getting sick like monthly or so, for a couple of years. Putting dozens of kids in a closed space for hours is something that just wasn't a thing in previous generations either.
So personally, yes, I would bet that chances for pathogen spread have increased greatly.
There are significantly more humans in which a human-borne virus could live and/or mutate.
There are significantly fewer humans living in close contact with livestock in which a zoonotic virus could be transmitted. I'm skeptical that there has been a net increase. It's possible but I haven't seen any reliable evidence one way or the other.
But there are significantly more amounts of livestock in contact with those fewer humans.
Think of it this way: more total numbers = more opportunities for viruses to grow or mutate = more chances for runaway or novel infections. Runaway infections are dealt with fairly well by government entities. Novel infections... might be harder to discover because they're, well, novel.
Agreed. We've had this immune system battling stuff non-stop throughout evolution and now we're living in these clinical environments and it's going haywire.
Not to mention we're poisoning ourselves with all sorts of novel stuff, especially poor hi-carb nutrition, ultra processed food and pollution from various sources that act as endocrine disruptors and God knows what else.
Time scale. Viral load has increased dramatically over what it was like 1000 years ago. The change over the past 100 years is all lifespan due to antibiotics and the sterility another comment is pointing the finger at. It’s possible that viral load + lifespan = cancer, dementia, autoimmune stuff, etc.
My girlfriend has Crohn's disease that can be directly correlated to food poisoning while on vacation. Now years later I can't even count the times I've read and heard exactly the same story from other people with Crohn's disease. A simple search for "Crohn's food poisoning" turns up hundreds of results. I can't believe this is not being investigated with higher priority
Another comment in this post mentions reactive arthritis and HLA-B27; there's some evidence suggesting "permanent" autoimmune conditions in HLA-B27+ people also might come from viral triggers.
most of those with crohn's would likely have developed it at some point - 99% of those with food poisoning won't develop crohn's
Can we take it as proven that the rate of these diseases has increased? I wonder if in the past some conditions we now classify as particular diseases were considered a normal part of aging, perhaps at most getting a blanket classification of “senility”.
Immunocompromisation due to chronic inflammation from dietary issues and stress in addition to the above as well
The frequently cited "stress" thing of modern lives is just eyebrows-raising. Do anyone actually believe that lives of people 100 or 200 years ago have been less stressful?
Physical activity gives an outlet to stress, and people used to get way more of it. Stress and physical effort are supposed to go hand-in-hand; you feel stressed, which gives you a boost of adrenaline, which you need to physically fight back whatever caused the stress. When the physical component is missing, the stress just lingers and wreaks havoc on your body.
Also, sunlight exposure (with limited UV) went hand in hand. Now we have neither.
Careful. Exercise also causes a stress response in-and-of itself.
I think the idea is that the cells are stressed due to inflammation due to diet, rather than psychological feelings of stress
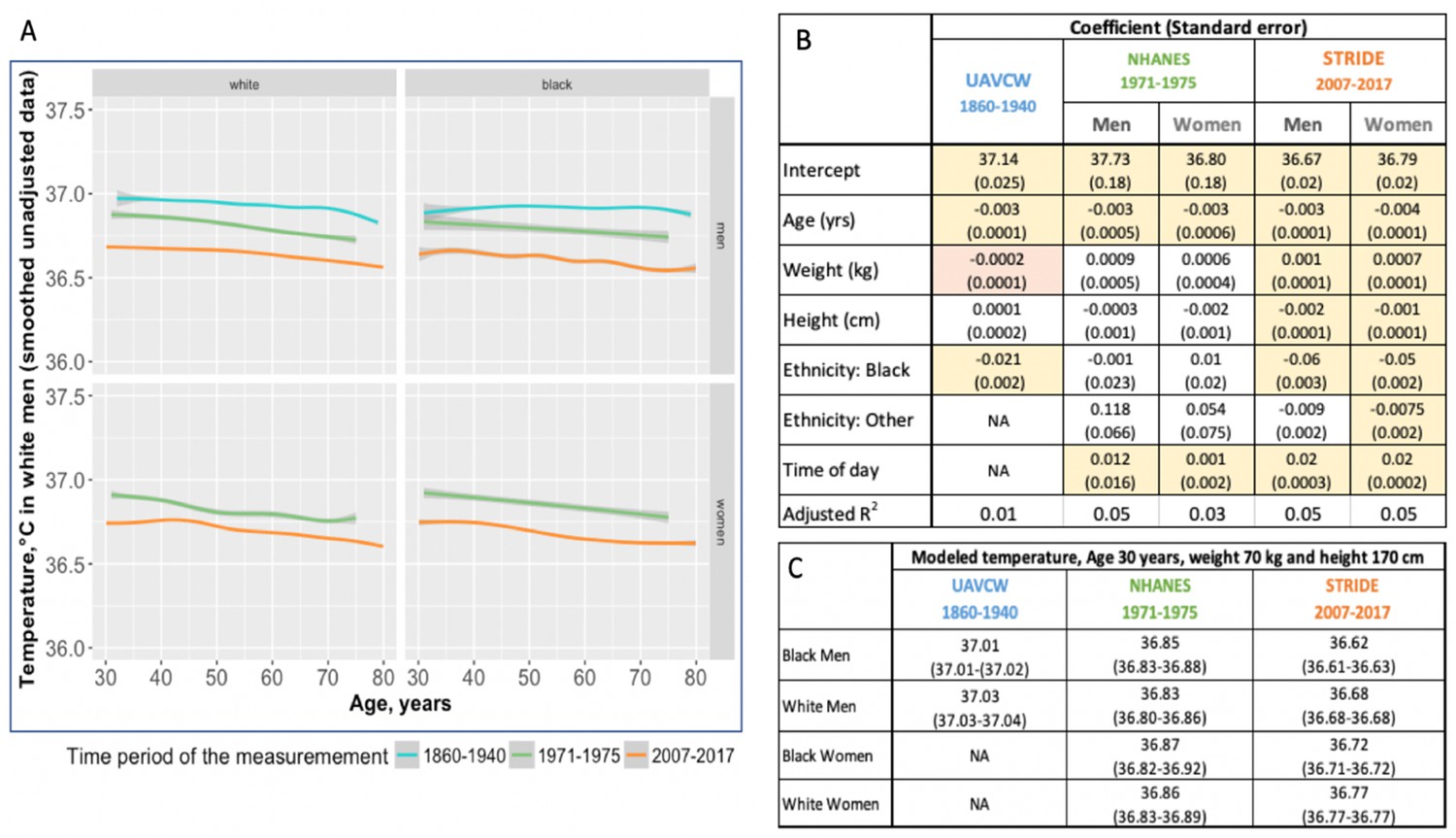
Average "healthy" body temperature is down more than half degree exactly because of reduction in inflammation. People used to have very unsanitary lives and were fighting infections nonstop. 37.0C was the "normal" body temperature when the "norm" was first discovered in the early XIX century, now it's considered to be a sickness already.
I'm not an expert but maybe keeping the immuno-army busy with constant infections keeps it from going bored and attacking itself
also not-an-expert opinion, but an average higher body temperature would reduce immune system workload by virtue of killing a lot of stuff dead via inhospitable environment before an immune reaction could ever muster..
Fascinating claim, where did you hear this?
It's possible they had better support systems due to larger families, church being more prominent, etc.
Any form of positive community is helpful, religous or not. Just having caring neighbors is a boon to well-being.
well, you may read & discuss this one? :)
https://en.wikipedia.org/wiki/List_of_common_misconceptions_...
Work is not the same as stress. People today (especially near the bottom of the ladder) are not in control of their own destiny like they used to be. It's a different kind of stress.
Slaves were more on control of their own destinys than someone working an entry job today?
I was thinking more about farmers.
I think there’s something to this. Life in those times was difficult and stressful, yes, but most hardships then were entirely beyond any individual’s control. To a large extent, good times and bad times would come and go regardless of what you did.
Contrast this to the modern day where more often than not, hardships are attributed to personal failings (“You should’ve worked harder if you didn’t want to be stuck working abusive under-compensated jobs!”) and people perpetually teeter on the edge of a knife suspended over a bottomless pit. If anything goes wrong, it’s treated as nobody’s fault but your own, regardless of the reality of the situation. It’s almost a type of psychological torture.
And they used to be more in control? Epidemics wiping out whole families? Gulags, concentration camps? Religious violence? Persistent threat of starvation death that was just the norm of life? One year of crop failures, and your kids are dead. Two years, and you are dead yourself. And it doesn't depend on you at all, just bad luck (if there was too much luck - like a generation without crop failures - population doubled, then just one year of crop failures meant you were dead). And yeah, the Church that keeps telling people that they were all sinners and will burn in hell, very comforting. Tell me about "control of one's own destiny".
Have you read Dr. Casey Means’ book on this?
Literally every time in the history of the universe when someone has structured a sentence like this, in this context, whoever they're talking about ends up being a giant crackpot. I'm not saying this person is a crackpot, just that the pattern recognition systems are throwing off some alarms.
If you end up dealing with a chronic disease that medical doctors completely fail in dealing with, you naturally get driven to look at “alternatives”. There’s a lot of nonsense out there - but some of it works. As a former skeptic I’m now much less dismissive of these things due to my own circumstances. Particularly when I can see that poor medical treatment over the years actually exacerbated my condition and being less skeptical could have improved my quality of life significantly sooner.
Now that you mention that pattern, I can’t say I disagree with your comment. However, the information I can find about Means seems to be fairly…non-controversial. Or at least I don’t understand the controversy (which is very likely).
First sentence from wikipedia says:
Casey Means is an American functional medicine/holistic medicine physician, entrepreneur and author.
I'm more influenced by this passage:
Means withdrew from her medical residency at age 30. She has attributed this decision to the lack of training she received about nutrition and the underlying causes of chronic disease. Means dedicated her practice to functional medicine, which focuses on the root causes of disease.
As one comedian said: “Do you know what they call alternative medicine that works? Medicine!”
Tim Minchin! (about 4 minutes in): https://www.youtube.com/watch?v=KtYkyB35zkk
that's cute but how much alternative medicine eventually finds a way into real medicine?
in other words : someone telling someone to practice yoga to relax and reduce their heart rate 200 years ago was a quack right up until the point that modern doctors decided to include it in their repertoire?
it's a cute joke but it skips over the fact that there seems to be an 'alternative medicine -> real medicine' pipeline, even if a lot of it turns out badly.
Medicine as a science didn't exist 200 years ago.
Breath exercises, and physical therapy for relaxation were mainstream in 1960-s.
> it's a cute joke but it skips over the fact that there seems to be an 'alternative medicine -> real medicine' pipeline
Not really. Most of the non-medicine (I refuse to call it "alternative") stays non-medicine: acupuncture, homeopathy, all the "energy meridians" nonsense, ayurveda, alkaline foods, etc.
And even with activities like yoga, it's not more effective than other types of similar physical activity. There is some very weak evidence that yoga _with_ physiotherapy might be more effective than just increased levels of physiotherapy.
The actual quote (from memory, but I just listened to the monologue a minute ago): "Do you know what they call alternative medicine that's been scientifically proven to work? Medicine!"
In other words, the quote is exactly referring to your "pipeline."
Tim Minchin's "Storm" monologue: https://www.youtube.com/watch?v=KtYkyB35zkk
Well that red flag versus the immediately-preceding passage listing a Doctor of Medicine degree at Stanford Medical School.
I looked into one of the links and apparently she pushes fairly mainstream preventive medicine stuff, diet, exercise, and screening tests. The only questionable thing I saw was the continuous glucose monitoring thing which the jury may still be out on when it comes to non-diabetics.
I haven't tried a continuous glucose monitor myself but those non-diabetics who have generally claim that it gave them interesting insights into how their blood glucose level reacted to different foodstuffs and timing of meals. There is a lot of individual variation there due to genetics, lifestyle, gut microbiome, etc. We'll probably never see a large-scale, long-term randomized controlled trial to show that CGM use improves health outcomes for non-diabetics. But for healthy people who already have the basics dialed in, a CGM can probably help them eke out some additional marginal gains.
And obesity.. there are several adenoviruses associated with it. Example: https://www.nature.com/articles/s41366-021-00805-6
(Although the article takes pains to say that obesity is multifactorial, conflicting evidence in humans, etc.)
Bacterial infections can also trigger autoimmune diseases - it's not just viruses.
Realistically immune systems are extremely complex and I suspect there are probably lots of environmental triggers beyond viruses and bacteria as well
{kind=link}
The part of these sort of conversations that makes me wary is this understanding that "Alzheimer's" is a disease with a single cause. I think it is beyond question that some viruses trigger Alzheimer's, because viruses can do pretty much anything. The real question that they're studying is to what extent do viruses cause Alzheimer's. If it turns out that most Alzheimer's cases are a Herpes symptom then that sounds big.
I agree, it is very frustrating. I will say that the reason they have not found a cause and/or cure for Alzheimer's is that it is a polygenic and polyenvironmental disease. The only way to cure Alzheimer's is to look at each person individually (personalized medicine) but that is expensive and not as profitable.
Do you have know of any individualized Alzheimers treatments resulted in the cure, slowing down, or "stopped further damage"? That would seem like big news, even if it was only in a person or two.
So then "curing Alzheimer's" is akin to "curing cancer". If this is true, I wish this truth was better disseminated.
Is the theory now that Alzheimer's just actual brain rot, of which their are multiple causes, and that beta amyloid plaques are just detritus of a losing battle?
We have built a rather large toolset for detecting and treating a range of cancer variants over the last decades. With meaningful changes in expected outcomes. Considerable drop in mortality, for example. Far from cured though. Alzheimer's might be much trickier. ..
I’m guessing it’s trickier because it’s harder to get biopsies of the brain mid treatment. It doesn’t help that it’s been treated as one disease and assuming a single cause for so long
Some researchers think Alzheimer's is a man made disease.
The last time I read up on this it was basically that we all have some predetermined risk of developing an Alzheimer's type disease, but that modern environmental variables raise that risk to such a high likelihood that it's become something it never used to be.
Interesting to think about.
> , but that modern environmental variables raise that risk to such a high likelihood that it's become something it never used to be.
Well, yeah, because more people get old enough to get it.
The way I've looked at it (and I work in the adjacent space of neurotech/sleeptech) is that it is likely we are assigning multiple diseases with the label of Alzheimer's because we don't understand the disease well enough.
I wouldn't say the question should be "to what extent do viruses cause Alzheimer's". I mean you could run a regression analysis to find that and then what?
The real question is what is going on and how do we fix it?
Along similar lines there was a good article in the Guardian: The brain microbiome: could understanding it help prevent dementia? https://www.theguardian.com/lifeandstyle/2024/dec/01/the-bra...
Apparently viruses and also bacteria and fungi getting in the brain and causing problems are quite common.
Can someone explain to me how it can be so hard to track down the exact cause for this disease? My grandma passed from it. It seems to be relatively common. What makes this so difficult to treat relative to other diseases? Freshman year of college I was told it was amyloid proteins. Then make a drug to eliminate them. I am having difficulty seeing how 20 years since my grandmother passed, the cause still shows as unknown on reputable sources.
We still don't have a correct model for what Alzheimer's is, and therefore how to treat it.
Compare this to something like HIV, where we were able to quickly understand that the virus attacks CD4 cells, and limits the body's ability to defend from disease.
With Alzheimer's, we're still in the - is it amyloid and tau? is it inflammation? is it viral?
This is compounded by our limited understanding of the brain.
Another hypothesis which I ascribe to is that we are lumping multiple diseases under the label of Alzheimer's because we don't understand it enough.
That's interesting. It could be multiple different dementia diseases that are different enough to require their own hypothesis. I recently read League of Denial: The NFL's Concussion Crisis. CTE is also a brain condition that is only diagnosed postmortem due to the invasive procedure needed. It seems the brains of living are indeed difficult to study.
I think another thing to consider is that we really don't know how the brain works. Sure we know there are neurons, and they create electrical charges, and there are neurotransmitters, etc etc. but we REALLY don't have a model for how these things relate to thought, memory, etc.
I equate it to how our understanding of the body has changed over time. When we understood fluid dynamics, we looked at the body as a series of pumps and magical fluid called blood which carried nutrients. When we discovered electricity, we slapped our foreheads, and thought "of course!! it's electric!!" and now we relate everything to our understanding of electrical activity AND hydrodynamics. I am sure there is a time in the not to distant future where we will discover how the mind works is related to our understanding of quantum...and we'll continue down the rabbit hole.
the brains of living people are difficult to study and test
"Alzheimers-like" is a thing too: https://www.research.uky.edu/news/uk-researchers-find-alzhei... (after covid). I am sure there were other studies, but I'm darned if I can find them after searching just now.
> Two other studies, one by GSK, a pharmaceutical company, and another by a group of academics in Britain, also reported that a newer “recombinant” vaccine, which is more effective at preventing shingles than the live version, appeared to confer even greater protection against dementia.
"confer" is something you use for a proven link with an interventional study, not for some random link you found within the thousands of variables you went fishing for in your observation study dataset.
Hence why the article does not say that the vaccine conferred protection against dementia, but rather that it appeared to confer protection.
appear to confer is a pretty biased wording. Rather, the only correct way to write about it is "there was a correlation that needs further investigation, we have no idea if there is a causal link about it".
I do not see the bias, all the more so given that the whole article after that first paragraph very clearly explains that further investigation is taking place to determine whether there is such a causal link. I have no idea whether conferring is a strictly defined term in the context of clinical research, but even if it is this is not a scientific journal article but aimed at the general public.
Going in detail to the claim that 'appear to confer' is biased, even if we take such a strict understanding of confer, compare the semantic effect of affirming and negating the sentence with and without 'appear to'
1. 'the vaccines conferred protection'
2. 'the vaccines did not confer protection'
3. 'the vaccines appeared to confer protection'
4. 'the vaccines did not appear to confer protection'
Which of the sentence above is closest to the truth, and which is most inaccurate?
thr vaccine study is a pretty clear (partial) causal link. there is a jump discontinuity in all causes dementia cases based on week of birth, where the jump occurs at the NHS policy cutoff week (if you are older than this week you are ineligible fof the vaccine).
It's likely partial because vaccines only confer resistance against one subset of virii and there may be nonviral Alzheimer's too. in any case causality is not really in question in that study
I agree.
Double blind randomized controled trial or it didn't happen.
Perhaps people with early symptoms are not given the vacine because it's too expensive and not mandatory?
Perhaps people with the vaccine are younger becase it's a recent vaccine?
Perhaps people that has no money for the vaccina had no money for therapies to slow the sympthoms?
Penultimate paragraph of TFA:
'The first double-blinded randomised clinical trial to test the effectiveness of antivirals against dementia is now under way. A group of researchers mostly based at Columbia University are testing whether valacyclovir, an antiviral used against HSV1, can slow down cognitive decline in people with early stage Alzheimer’s. Between 2018 and 2024, the researchers recruited 120 patients and treated half with the antiviral. They expect to publish their findings later this year. John Hardy, whose research forms the basis of the dominant amyloid theory of Alzheimer’s, and who has been a critic of the virus theory, says that a positive result in this trial would begin to convince him otherwise. If Dr Geldsetzer and his team can secure the funding, a similar trial of the shingles vaccine may soon follow.'
Oh wow, a bunch of Alzheimer’s grants at Columbia were canceled, including the Alzheimer’s Disease Research Center. Unclear if this study was affected…
https://taggs.hhs.gov/Content/Data/HHS_Grants_Terminated.pdf
So... and unfinished RCT of an unrelated drug an a project to start in the future a RCT of this new use of the vaccine.
The problem is mixing the real protection of the vaccine against shingles that has been tested in RTC and new aplications that have not been tested enough.
If there are too many false provisional anouncements, people will not thrust medicine.
The article opens describing how people vaccinated against the HSV1 virus are statistically less likely to develop dementia, and that a newer virus appears to confer an even bigger effect.
The article then proceeds on the history of the scientific debate on whether the HSV1 virus has a causal link to Alzheimer's and the level of acceptance of the hypothesis.
Finally, the article concludes describing how an RCT is taking place to find whether an antiviral which is used to treat HSV1 has an effect on the development of dementia.
It all ties together with the theme of the article, which is about the possibility that viruses may trigger Alzheimer's and the reason why research is being carried out in that direction. That open question is literally expressed in the headline.
I honestly cannot understand the problem you are seeing in the article. How else would you express the same information?
> Double blind randomized controled trial or it didn't happen.
This is just cargo culting. Read the original source paper and you'll understand why the causal relationship makes sense without an RCT.
Do you have the DOIs?
I found https://www.nature.com/articles/s41591-024-03201-5
They compare people that got the old vaccines in 2014-2017 with people that got the new vaccine in 2018-2020. Some strange parts:
They say they are analyzing 6 years, but for the second group the 6 years period has not ended. This makes the comparison difficult.
These periods includes the covid-19 epidemic in 2020, with lock downs, changes in death rates and new vaccines. This makes any comparison difficult.
The comparison in figure "1 e" have very different initial slopes. I'd expect dementia to be a slow accumulation of small problems in the brain, so I'd expect an initial equal slope and after some time a difference. They start the comparison after 3 month, but I expect a slower effect.
Figure "1 f" has the same initial slope difference, but there is also a strange slope change in d=1750 and the red line is more noisy probably due to the unfinished 6 years period).
Preprint of the main paper on pubmed: https://pmc.ncbi.nlm.nih.gov/articles/PMC10246135/
They rule out the objections in your top post — as well as whether people chose to get the vaccine, which would be a huge confounder for a disease that affects cognition.
In your link, they also cut at 2020 that is very difficult to compensate in a comparison.
Double blind randomized controlled trial with endpoints and statistical methods disclosed in advance from a lab with a reputation for publishing null results, or it didn't happen.
Wouldn't this theory be easy to prove by sequencing brain tissue samples from deceased patients?
Probably more than 90% of the reads would be human, but still.
Do we really need questions as headlines?
It's bad enough that people fail to contextualize or deeply consider the reality behind sensational headlines, but when you open the door to vague questions as headlines, you are somehow journalistically allowed to memetically plant a known lie into the zeitgeist of the majority of internet users who read the headline but dont click to read the article.
I would agree if the article was an example of Betteridge's law of headlines [0], but in this case it is legitimately reflecting the overall message of the article, which is that it is becoming an open research question in science whether viruses trigger Alzheimer's having previously been a fringe hypothesis.
The very fact that the last sentence of the article is expressed as a conditional is also consistent with the use of a question for the headline:
> 'If antiviral treatments can indeed slow, delay or prevent even a small subset of these cases, the impact could be tremendous.'
[0] https://en.wikipedia.org/wiki/Betteridge's_law_of_headlines
If there is no scientifically meaningful finding there is nothing to write about. You may as well write "do unicorns go around sprinkling Alzheimer's healing dust at night?"
It's an open question, surely worth writing about and getting people's attention on right? No? Right because scientifically meaningful distinctions are the only way to understand underlying scientific process.
This is not philosophy class.
Is there tantalising evidence suggesting that unicorns may go around sprinkling Alzheimer's healing dust at night? Have scientists who were previously sceptical of the unicorn-Alzheimer hypothesis now become open to the possibility? Are clinical trials that may provide evidence in favour the causal effect of unicorns on Alzheimer's currently taking place?
That would very much be a very interesting news article, and I hope it is published.
We don't need them but I don't see a problem either if they are appropriate to the article as in this case.
It's really surprising that with all the statistical tools we have, the signal for the link between a common virus and a disease is unclear. Even if the road to a proven intervention is long, you'd think at least the link would be clear.
Once I started learning more about biology, I realized that everything is just so complex. The body repurposes chemicals a lot, so you have things like serotonin being a key neurotransmitter in the brain, but also in the gut. And you have enzymes that are coded in genes, but then there are also networks of genes that are up- or down- regulated by hundreds of other genes, and sometimes only in certain types of cells or certain physiological environments. And then of course there are epigenetic and immune-modulated effects at the genome, gene network, and individual gene levels. Not to even mention all the feedback mechanisms and meta-feedback mechanisms (the drive toward homeostasis is POWERFUL), and effects of countless chemicals in our environment.
There are certainly clear-cut cause-effect relationships in biological systems, but even they will have edge cases and random chance to muddle the picture.
I would posit that the human body is far more complex than even the largest codebase, not least because it was jury-rigged together with no architect or style guide.
Also, in general, the more common the exposure, the harder it is to find a link; try finding a control group of people who have never been exposed to PTFEs, or HSV, and who also aren’t like hunter gatherers.
My favorite way of describing biology comes from another HN comment:
> It’s more like a vibrating causal cloud than a chain of causality.
The problem is simply observational. We don't even have reliable DNA and RNA sequencing of our own bodies. And we cannot reliably observe things in a host without knowing, to some extent, what we're looking for first. Even that space is so large, it's very hard to ascertain accurately. Biology is always suffering for lack of clear observations.
Also, adding complexity is the difficulty or even literal impossibility of observing the direct interactions of elements of the system, which operate at a quantum scale, that you would disturb and do disturb when attempting to observe.
"Everything in biology is more complicated than it looks."
DNA is where we get our physical attributes (modulo environment).
No, a lot of DNA is "junk," i.e. we don't yet understand what it does.
No, a lot of functional DNA is turned on or off by the epigenome.
No, a lot of our metabolism is affected by our biome — thousand of species of bacteria that turn up or down various reactions, or produce other chemicals that we need...
It's not that we haven't thought up the statistical tools. The core theoretical tools you need are there. It's that gathering the data that you need is extremely difficult and time consuming.
If you gather EHR or medical claims record data for vaccines for example, you have to take very seriously the biases and impact of missingness inherent in the data. Is that person you have no evidence of disease for truly not diseased or do they just have missing data? IS it missing because they just didnt go to the doctor because they're healthy enough to kick the disease on their own or because they're so financially unstable that they can't afford to consistently see their primary care doctor. Is the data missingness itself actually what's more correlated with the disease than the vacciation you are looking at?
Example: If your outcome is dementia then may be using cognitive tests that have a high level of variability due more to social class, education, test taking ability. Is receiving a fancy vaccine is more likely in an affluent area? Could be that correlation itself might completely explain away the positive effect that vaccine has on cognitive test scores.
In Alzheimer's you're often trying to correlate things that happen in early life with long term damage that only surfaces many many years later. Retrospective studies where you go back and ask sick or healthy people have recall bias where the sick ones remember more issues with themselves early on than healthy ones do even with the same early life issues.
Not trying to say epi is perfect or that there isn't room for improvement in tools (there absolutely is). But just like often happens when crossing over into the biological sciences there's a lot stickier problems than people outside the field realize.
Right, the data quality is usually crap. Beyond the issues you mentioned, patients often switch providers or health plans and their data doesn't get migrated. In the USA at least there is no centralized national repository for that data so the further back you try to go the more likely the data will just be missing (or incorrectly coded). In theory there are interoperability APIs and national networks to solve this problem but in practice a lot of systems still aren't properly connected.
For vaccinations specifically the CDC Immunization Gateway can be a good place to start. Most states also maintain their own immunization registries that can be queried through standard HL7 V2 Messaging and/or FHIR APIs if you have the appropriate permissions.
The issue is that we don’t have the primary data. This stuff is messy and the systems at play are extremely complicated. Often one of the most challenging parts of bio sciences is figuring out a test that will cleanly show a result that is true.
Without directly testing for a connection it’s extremely rare to get unexpected data that confirms an alternate hypothesis.
Even if the statistical tools are there, they can’t make up numbers that we haven’t collected yet.
With Alzheimer's, it's possible that it's fraud hiding the linkage.
E.g., https://www.science.org/content/article/potential-fabricatio...
https://www.science.org/content/article/research-misconduct-...
https://arstechnica.com/science/2024/07/alzheimers-scientist...
https://stanforddaily.com/2023/02/17/internal-review-found-f...
> Authors sometimes share those with researchers conducting similar work, although they usually ignore such requests, according to recent studies of datasharing practices.
If the research was in anyway paid for with federal dollars all this data should be public. Not only that, if true it is a waste of federal dollars.
It's probable that the widening mistrust in science is due to this a sort of behavior and the resulting administration.
Waste due to inefficiencies is one thing, waste due to fraud, data hiding, misdirection is something else.
I think the link has shown up in the statistics for a long time. The article mentions Ruth Itzhaki being on it for 40 years. But things seem delayed by something along the lines of politics/corruption, or by the complexity of the situation with HSV1 not being the only cause. It can become a mess https://www.nytimes.com/2025/01/24/opinion/alzheimers-fraud-...
I'm hoping that AI helps sort this stuff out. It can read the papers and say hypothesis A is most likely even if professor Y had built an empire on it being hypothesis B.
HSV1 is estimated to affect more than 80% of the population, but less than 80% have dementia. This seems to imply there are other factors at play. Maybe it requires other factors like genetics or immune issues for it to progress.
I can't point to a citation but I'm sure I've seen it hypothesized that it requires both the infection, then some sort of injury to allow the virus to cross the blood brain barrier.
Or maybe they come through with the microplastics.
The article clearly explains that the link isn't clear at all.
It's that certain damaging proteins are a line of defense against the HSV1 virus, that something sometimes sends those proteins into overdrive, that this is influenced by genetics broadly, further influenced by a particular gene, and that it's a second infection with shingles that can reactivate the proteins, worsening it.
Given that this is the interplay of something like at least 5 factors, and there may be more, it's not surprising it's taken this long to put together, even with all our statistical tools.
The part that might not be clear could be due to other factors, such as a genetic or lifestyle component that cause this to only progress to disease in some individuals.
and 20ish percent of autism. See maternal immune over-activation.
This is why methylene blue has been so successful in Alzheimer's research. It's antimicrobial and gets into the brain easily.
By "so successful", do you mean "failed all pivotal clinical trials"?
I checked the Wiki page. There is a whole section for the quacks: https://en.wikipedia.org/wiki/Methylene_blue#Society_and_cul...
the debunked theory that certain diseases like alzheimer's and autism are caused by viruses cannot be true because that would mean that they are caused by inflammatory insult and that would mean that vaccines contribute to or cause certain diseases. this is dangerous thinking and should not have a platform anywhere
> the debunked theory that certain diseases like alzheimer's and autism are caused by viruses
No. Not only is it not "debunked", it is not even "a theory".
> cannot be true because that would mean that they are caused by inflammatory insult
No. Something being caused by a virus does not imply that the mechanism is "inflammatory insult".
> and that would mean that vaccines contribute to or cause certain diseases
No. That certain viral infections may cause ill effects by means of inflammatory processes does not imply that "vaccines contribute to or cause certain diseases".